
Copyright 2026, American Health Law Association, Washington, DC. Reprint permission granted.
The Centers for Medicare & Medicaid Services (CMS) finalized its calendar year (CY) 2026 Medicare Physician Fee Schedule (MPFS) on October 31, 2025 (2026 MPFS Final Rule), which introduced several key changes such as an efficiency adjustment, a bifurcated conversion factor, updates to practice expense methodology, and expanded opportunities in primary care and shared savings. Several updates in the 2026 MPFS Final Rule could affect physician compensation, with three changes standing out as particularly significant.
The Efficiency Adjustment
A critical component of the 2026 MPFS Final Rule is CMS’ finalization of an efficiency adjustment, designed to reduce work relative value units (wRVUs) for 91% of physician services. Evaluation and management (E/M) services are not impacted by the efficiency adjustment, which limits the effect on providers whose work is primarily visit-based. The reduction is instead directed at non-time-based services, resulting in a larger impact on procedural specialties that rely heavily on these current procedural terminology (CPT®) codes. This change potentially reflects CMS’ belief that many non-time-based services will be rendered more efficiently over time compared to time-based services like office visits. Given many physician compensation models rely on wRVUs as the primary productivity measure, this adjustment may require a reassessment of existing compensation models.
This downward adjustment lowers the effective Medicare reimbursement that clinicians practicing in the affected specialties receive because of decreased wRVU credit while maintaining the same work volume. Additionally, many physician and group contracts establish productivity bonuses or base salary floors tied to productivity. As a result of the efficiency adjustment, procedure-focused specialists may see reported productivity differences despite unchanged clinical volume and effort, which could impact provider compensation under existing contract terms.
While the exact degree of impact is expected to vary by specialty, service mix, and compensation model structure, this adjustment introduces a structural shift that organizations should be aware of. The table below summarizes how the efficiency adjustment may affect total wRVUs for selected surgical and hospital-based specialties based on the top 25 CPT codes by volume from the 2025 MGMA Procedural Profile Survey.
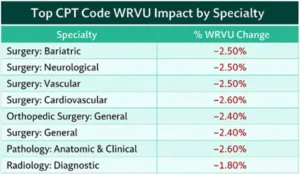
The analysis shown above reflects the estimated impact of the efficiency adjustment only and may not reflect additional wRVU adjustments from the 2026 MPFS Final Rule.
The Changes to Practice Expense Methodology
The 2026 MPFS Final Rule introduced a new practice expense (PE) methodology that fundamentally alters how overhead costs are calculated and reimbursed. Although the PE methodology has relied primarily on the American Medical Association’s (AMA’s) Physician Practice Information (PPI) survey data, CMS rejected the AMA’s updated PPI survey data because of methodological concerns, instead implementing a policy that dramatically diverges payment based on the practice setting. This new policy reduces the indirect PE allocated per wRVU by 50% for facility based services, recognizing the hospital or facility already covers such expenses.
This change reflects CMS’ view that providers incur higher indirect costs in office-based settings than in facility settings, aiming to eliminate what it considers duplicative payments for indirect expenses in facilities. Consequently, physicians performing services in facility-based settings will see lower reimbursement for those services, while office based services may see a slight increase.
CMS implemented the revised PE methodology on a budget-neutral basis: While total Medicare spending remains the same, reimbursement shifts from facility based services toward office-based services. This redistribution advances CMS’ broader effort to promote greater site neutrality across care settings.
Because of these changes, compensation rates, thresholds, guarantees, and professional services agreements tied to wRVUs should be recalculated to reflect current reimbursement economics.
The Bifurcation of the Conversion Factor
For the first time since the MPFS was established in 1992, CMS has implemented separate conversion factors based on participation in Advanced Alternative Payment Models (APMs), resulting in two distinct Medicare conversion factors. While the difference between the two conversion factors is modest, organizations with a combination of APM and non-APM providers may want to review their compensation processes and models to maintain consistency across their workforce.
Organizations using two separate conversion factors for APM and non-APM clinicians may necessitate separate Medicare revenue forecasts, particularly when paired with similar CMS policy initiatives, like the efficiency adjustment and practice expense methodology changes. Additionally, organizations with contracts that set payment as a percentage of Medicare may want to specify which Medicare conversion factor applies. While not all organizations may feel the immediate effects, these shifts are significant enough that awareness of the potential impact is necessary.
Preparing for 2026: Physician Compensation & Reimbursement Planning
These three policy changes introduced in the 2026 MPFS Final Rule may seem minor; however, when considered as part of the larger picture, they have the potential to significantly alter clinical productivity measurement, compensation plan methodologies, and broader financial planning activities. These changes demonstrate how important it is for organizations to understand how the reimbursement mechanisms that support their operations continue to evolve, and ultimately how these changes impact their workforce and finances. Proactive, thoughtful planning of compensation methodologies, productivity benchmarks, and contractual assumptions will help organizations position their physician compensation strategies for success throughout 2026 and beyond.
![]()
References
Medicare Physician Payment Schedule for 2026, 90 Reg. 49266 (Nov. 5, 2025) (to be codified at 42 C.F.R. pts. 405, 410, 414, et al.).
Med. Ass’n, 2026 Medicare Physician Payment Schedule and Quality Payment Program Final Rule Summary and Analysis (2025), https://www.ama-assn.org/system/files/2026-mpfs-final-rule-summary-analysis.pdf.
MGMA DataDive Procedural Profile, Medical Group Management Association, https://www.mgma.com/datadive/procedural-profile.






