2022 Not-For-Profit Health System Performance Trends
November 10, 2022
Written by Quinn Murray and Ed McGrath
Not-for-profit health systems nationwide are experiencing material financial pressures as the industry recovers from the impact of the COVID-19 pandemic. Now providers are faced with the difficult task of adjusting to the new challenges that healthcare systems are experiencing in 2022. The VMG Health Strategic Advisory Services team works primarily with not-for-profit systems, which is one of the reasons we decided to complete this report and the associated analytics. A consistent theme in this study finds that few organizations have been immune to material declines in financial and operational performance in 2022. This performance is not sustainable for the long term.
In addition to the costs associated with labor, supply, purchased services, and other inflation pressures, not-for-profit healthcare systems are also experiencing increased competitive threats. These threats are coming from niche players supported by private equity and other financially backed organizations that are typically focused on more profitable commercial business instead of serving all, which is the historical tradition of not-for-profit healthcare systems.
This report is based on data from publicly available sources and represents a statistical sample size of various organizations across the nation, but with that said, our findings may not be applicable in all markets. However, the organizations reviewed for this report represent a large cross-section of not-for-profit health systems in the country. The composition of these systems is summarized below.
On a combined basis, the 21 systems analyzed as part of this study represent $184 billion in total operating revenue for fiscal year 2021. A significant portion of this total was generated from the systems operating 560+ hospitals with approximately 100,000 beds across 32 states.
Other advisory firms have also noted recent declines in industry performance. The contributing factors identified by other firms are wide-ranging, some of which are consistent with the findings of this report.
For example, KaufmanHall reported in September 2022 that for the first six months of CY 2022, hospital operating margins declined 100% compared to 2019 before the pandemic. In addition, KaufmanHall noted the number of hospitals with negative margins in 2022 is projected to be greater than pre-pandemic levels since hospital margins continue to be consistent with, or worse than, 2020 levels.
Another example from RevCycleIntelligence from July 2022 cited survey results from over 200 CFOs of health systems and large physician groups. The results indicated that only 8% reported they were on track to exceed 2022 goals. Additionally, RevCycleIntelligence noted hospitals and health systems are experiencing increases in volumes and patient revenues. Research completed for this report is consistent with the findings noted in the RevCycleIntelligence article.
As noted, the factors driving poor financial performance in 2022 are wide-ranging. Discussions with management for purposes of this report have indicated that some of the issues include the following:
Contract Labor – Many VMG Health clients have been successful in managing contract labor costs due to reductions in hourly rates. Others are reducing clinical capacity, including beds, to minimize travel and agency staff needs.
Employed Staff Labor Costs – In order to attract and retain staff during increased market pressures and demand, systems are implementing pay raises well above traditional industry norms. Based on our research, this is expected to continue going into 2023. Conversations with the management of various systems included in this report indicate planned salary increases of 4% to 8% in 2023.
Medical and Other Supplies – Recently, systems have experienced material increases in the cost of goods purchased and services purchased by these systems. The calendar year 2023 expectations from VMG Health clients indicate planned increases of approximately 6% or greater, which would be materially higher than traditional industry norms.
IT and Other Support Services – Beyond clinical staff, market competition also exists for IT and other support staff who are in short supply. This is another contributing factor driving up the cost for health systems.
Medical Malpractice – As a result of cases being delayed for the greater parts of 2020 and 2021, clients are beginning to experience increased malpractice activity from cases during this time period. This is leading to increased malpractice costs which are rising to levels that may have not been anticipated.
Key Findings & Conclusions
The findings and forecast based on this report do not necessarily paint a pretty picture for not-for-profit systems. While our research is focused on healthcare systems, VMG Health’s experience with standalone hospitals in 2022 also indicates, in most cases, financial performance is weaker than what is being reported for several other systems.
Of the 21 systems analyzed for this report, in calendar year 2022, 16 are reporting negative operating margins (75+%). The other five are reporting breakeven or very minimal operating margins. Each of these systems reported positive FY 2019 operating margins before the pandemic.
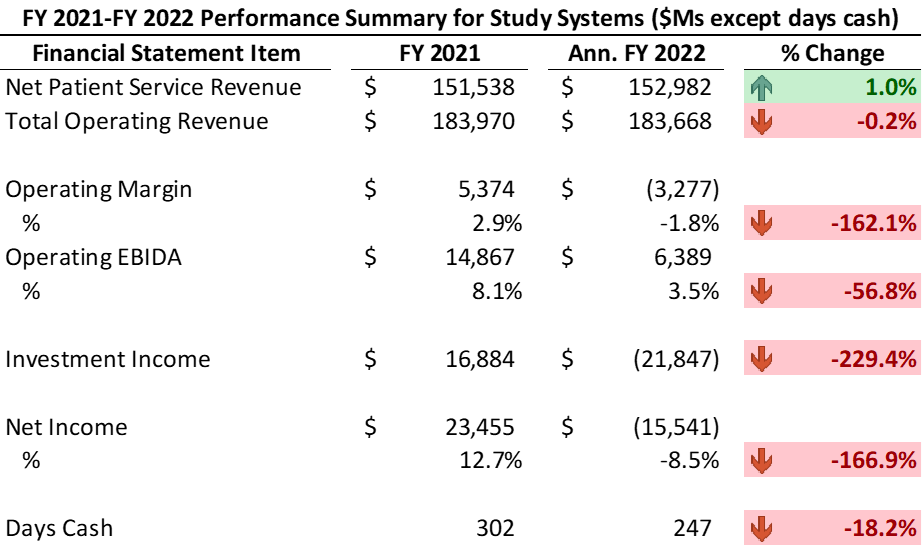
The range of the operating margin declines in 2022 as compared to 2021 and/or pre-pandemic levels approximates from 4.0% to 7.0%. In other words, if the operating margin was a positive 2.0% in 2021, then the 2022 operating margins will likely approximate between -2.0% to -5.0%. Likewise, operating EBIDA for these systems has deteriorated materially to approximately 3.5% of total operating revenue in comparison to 8.0% in 2021 before the pandemic.
Similarly, these systems have experienced a significant decline in days cash, specifically in 2022, approximating -18% from 2021. The systems have also experienced material losses from investment income in 2022. Recognizing this mostly includes unrealized losses, these systems reported investment losses of approximately negative -$22 billion on a combined basis.
Summary Performance Results from FY 2021 to Annualized FY 2022
Negative operating margins in addition to poor investment performance (and other non-operating activity for certain organizations) are driving declining cash balances. 2022 performance indicates systems reporting somewhat material declines in days cash on hand. These 21 systems are reporting a 15% to 25% decline in days cash with an average of an 18% decline from fiscal year-end 2021.
As an additional consequence of the material losses, especially for smaller systems, debt service coverage ratio (DSCR) covenants may not be met. Most of the systems included in this report have the cash reserves necessary to avoid procedural requirements relative to the days cash covenant in their bond agreements, and this includes taking into account the poor 2022 performance.
Organizations in 2023 may be required to develop a financial improvement plan outlining the recovery path to fulfilling the DSCR covenant in a subsequent fiscal year. In many cases when a bond covenant such as DSCR is not met, systems are required to hire management consultants to report on their opinion relative to the likelihood the system can meet the DSCR threshold in the near term.
VMG Health recently completed one of these assignments for a large hospital in the northeast. Based on this assignment and discussions with others, based on 2022 performance it appears other organizations will unfortunately need this type of study completed by experts such as VMG Health.
Areas of Consideration – Initiatives to Address the Impact of 2022 and Beyond
It is clear most organizations will not be able to shrink their way to success, and over time, strategic growth is imperative to long-term success. The following are example actions either undertaken or being contemplated by VMG Health clients to address recent performance:
Addressing care management issues to better utilize limited clinical care resources.
Increased focus on APP utilization to the max of their skill levels.
Enhance utilization of scarce clinical staff resources.
Digital care to increase patient access at a lower cost.
Expansion of remote monitoring and other vehicles to reduce more expensive utilization.
Expansion of hospital-at-home services.
Assessment of the value proposition of employed/aligned medical groups.
Identification of how best to maximize the group size, strength, and the system’s investment in the group.
Contract negotiations with managed care payors.
Will likely be difficult to obtain increases that will address inflation pressures.
Strategic assessments of existing operating assets/investments.
Reevaluation of the continuation of existing service lines.
Closure and/or sale of hospital assets in non-strategic markets.
Disposition of unprofitable ventures that are no longer strategically imperative.
Reassessment of the need for existing real estate and/or MOBs.
Evaluation of the potential sale of other non-core assets.
Operational improvements.
Reducing bed and other capacities to match available non-agency/travel staff.
Identifying opportunities to improve revenue cycle efficiency.
Staff modifications, primarily in non-clinical areas.
Acquisition of organizations that are struggling.
Based on discussions with VMG Health clients, systems are being more diligent relative to making investments in new facilities.
Partner/affiliate with other systems for non-clinical services.
Example areas include IT, revenue cycle, cybersecurity, analytics, and others to improve cost efficiency and reduce potential future investments.
Price transparency.
Summary
Not-for-profit healthcare systems are experiencing extreme challenges in 2022. Based on conversations with many of these organizations and other clients, this is unlikely to improve materially in 2023. Not-for-profit hospitals and systems need to explore other innovative avenues to work smarter and more efficiently so they can be well-positioned for success in the future. VMG Health has a history of experience developing long-term relationships with clients through providing assistance across a variety of areas. These areas primarily consist of financial and strategic related assistance, which has prepared and positioned VMG Health to provide support and insight to not-for-profit hospitals and health systems. As we continue to assess the not-for-profit landscape, VMG Health has the experience to add value and help systems address some of the issues outlined in this report.
The assistance VMG Health’s experts are able to provide can take many forms. Some examples are:
Behavioral health is a highly fragmented market. With an increased demand for providers as well as the recent supply shortage, this sector requires innovative partnerships and strategic thinking.
Here are the top three strategic issues in behavioral healthcare to consider currently.
1. Provider Availability
Most health systems and provider groups struggle to recruit and retain enough psychiatrists to meet community needs. In many cases, a lack of provider resources limits the growth of existing services or prevents clients from offering a behavioral health program at all. Residency programs or other less formal relationships with medical schools have proven to be effective recruitment tools.
2. Fee-For-Service Economics
From a contribution margin and net income perspective, behavioral health services are well below average for many health systems. This is largely due to some combination of the following:
Payer mix: For example, disproportionate share of Medicare, uninsured, etc.
Reimbursement rates.
State policy and community resources: Health systems are often required to use upwards of 25% of their capacity to board behavioral health patients due to a lack of community post-acute options. Patients no longer meet the criteria for inpatient reimbursement.
Organizations assuming higher levels of financial risk generally favor the economics of behavioral health due to the service line’s impact on the total cost of care. This phenomenon has resulted in increased interest and investment in behavioral health for many clients. VMG Health’s advisory clients have recently identified behavioral health as one of the most important service lines moving forward.
3. Care Model
The care model needed to provide behavioral health continues to be an area of interest for many organizations. Clients are increasing investment in pre-inpatient and post-admission services and community resources to improve program performance.
Organizations are revisiting medical group strategy and physician alignment in the face of private equity investment, growing medical group losses, and a decline in overall performance. Approaches on how to address medical group performance vary but can broadly be categorized as performance optimization (i.e., enhancing the current alignment vehicle) or pursuing a structure change to an existing model that improves sustainability. In lieu of performance-focused optimization, organizations are increasingly considering whether there are alignment models that are more sustainable and functional than traditional employment given the price transparency and site neutrality trends. The following article explores the evaluation of current medical group performance.
More health systems are taking a multi-faceted approach to maximize medical group performance. The exponential growth in physician and advanced practice provider employment and the growth in reimbursement tied to cost, quality, and access have heightened the importance of medical group strategy. However, many organizations continue to experience underperformance across several domains (cost, growth, access, etc.), and attempts to improve performance have stalled or been met with significant resistance. In most cases, the definition of performance is too narrow to identify the actionable strategies necessary for improvement.
Measurement of medical group performance and provider efficiency has historically been based on investment or operating loss per physician. In VMG Health’s experience, questions pertaining to a medical group optimization are complicated and require consideration of several indicators. Commonly used measures like investment per physician and provider FTE are helpful but can be misconstrued without proper context due to a myriad of factors. Some of these factors include but are not limited to medical group provider composition (e.g., primary care, hospital-based, pediatric subspecialties, etc.), medical group structure, care model, payor contracting strategy, overhead allocation, and payor mix.
To truly understand medical group performance, performance should be evaluated across a series of clinical, financial, operating, and community domains to ensure the group’s value is fully realized and understood. Focusing on only one or two aspects of medical group activity can result in an overly narrow and often inaccurate assessment of medical group value. The approach to assessing the economic sustainability/affordability of a medical group should be based on a complete picture of the medical group’s impact on health system financial performance and should not be limited to a simple financial review of practice operations.
It is critically important to consider how the medical group functions, performs, and contributes to the health system in several areas including: 1) growth trajectory and overall affordability, 2) engagement of the provider group, 3) data availability and reporting, 4) provider care model and compensation, and 5) provider governance. Strong performance across one or two domains is not indicative of sustainability and category weighting is required to acknowledge the relative importance of each.
Each of the domains can be evaluated and indexed across several factors to essentially score the medical group’s overall health and determine whether financial, strategic, and clinical alignment requires modification for sustainability.
Performance Domains
Affordability
The affordability domain evaluates the extent to which the magnitude of the hospital or health system’s investment in the medical group is appropriate given the size, operating performance, structure, and breadth. The domain also considers whether the investment is financially sustainable for the organization when tested against the parent organization’s size, operating performance, and market conditions.
VMG uses a wide array of metrics to measure affordability, including but not limited to metrics that measure the enterprise-wide impact of employing physicians. Depending on organizational compliance and internal firewalls related to information sharing, our preference is to develop management models that combine enterprise-wide economic contribution to the underlying net investment in the professional practice.
Without a common understating of enterprise-wide performance, medical groups are all too often in the position of defending their status in a health system. Further, our experience suggests there is increased dissatisfaction among providers and operators.
Engagement
The degree to which medical group infrastructure and policies support physician-to-physician and physician to group accountability. The engagement domain evaluates whether policies support the individual or the collective, and to what extent the governance structures create peer accountability and a set of medical group values that align with health system goals and objectives.
Data Reporting
The ability of the health system and the medical group to track, report (internally and externally), and act on data is essential. Supportive data systems, with actionable dashboards and reports for providers, are deployed to maximize the utility of the group practice. Medical groups lacking effective data tracking, reporting, and management capabilities are extremely limited.
Care Model
Exponential growth exists in patient care delivery in non-traditional settings and by care teams versus individual providers. What policies, procedures, and models have been developed and implemented that support care innovation, efficiency, and patient access? How well developed are virtual protocols and how mature is the medical group’s thinking about advanced practice provider utilization and deployment? Does this translate into aligned remunerations systems for providers?
Governance
The governance domain assesses how decisions pertaining to medical group management and operations are made as well as who is making the decision. There is not a one size fits all approach to organizational structure and decision making. What structures and policies support provider-led management and decision-making? To what degree are service line management and medical group operations integrated to assure efficient and effective operations.
Conclusion
Completing an internal assessment across these domains will benefit the medical group and the broader health system clinical enterprise. Completing this type of assessment generally assumes arrangements are fair market value and commercially reasonable, however, there is some inherent connectedness between affordability and internal compliance standards. Since the inception of the Stark Law in the late 1980s, there have been concerns about the commercial reasonableness of physician practices that lose money. While most operators could rationalize why practice in a health system model may lose money, there have been decades of discomfort with the strict interpretation of the Stark Law. In the most recent changes to Stark, there has been a clarification noting that the determination of an arrangement’s commercial reasonableness does not turn on whether the arrangement is profitable. Under the statute, there are several examples of community need, EMTALA, charity care, and quality that may support underlying commercial reasonableness despite practice losses. Nevertheless, assuring internal compliance policies and oversight are contemporary with the current law is paramount.
In VMG Health’s experience, questioning medical group sustainability is both essential and complicated. Many organizations struggle with assessing current performance in a way that provides a comprehensive view and provides actionable strategies for improvement. It is critical this work effort is organized in the right way since a simple benchmark exercise is largely ineffective in driving change.
Five Key Takeaways From the Public Healthcare Operators in 2021
February 9, 2022
By: Olivia Chambers, Savanna Dinkel, CFA, Madison Higgins, Madeline Noble, and Ayla Saglik
As we enter 2022, we look back to reflect on the major trends that shaped the healthcare sector over the past year. COVID-19 continued to be a major player throughout 2021, forcing healthcare systems to adapt to new variants, rising labor pressures, financial activity, and new regulations. Despite these challenges, the sector remains optimistic and ready to adapt.
Here are five key takeaways we believe defined the healthcare sector over the past year:
Financial Recovery From Pandemic
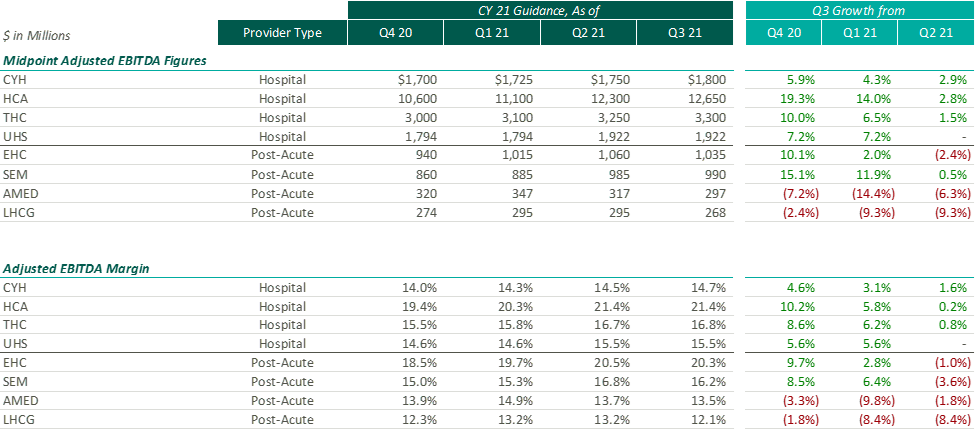
After the Q2 earnings season, VMG Health released an article analyzing post-COVID healthcare operator guidance. Generally, we found that healthcare operators were optimistic about the recovery of their revenue and adjusted EBITDA metrics over pre-pandemic levels, with most operators increasing their FY 2021 guidance with each subsequent reporting period.
While optimism for recovery to pre-pandemic levels remains, it appears that the post-acute operators have tempered some of their recent growth expectations. Based on disclosures of the public operators, the recent resurgence of COVID-19 through the Omicron variant has caused additional strain on the post-acute sector. During the J.P. Morgan Healthcare Conference, Universal Health Services (“UHS”) CFO, Steve Filton noted that the company was struggling to find providers who can accept COVID patients once they are ready to be discharged from the hospital.
Post-acute providers appear to have been hit especially hard by the recent labor shortages in the healthcare industry (discussed further below). As compared to the hospital operators, the financial performance of these post-acute providers has been affected disproportionally by the labor shortages. While hospital operators have been receiving additional reimbursement for COVID patients, helping to offset a portion of the increased staffing costs, the post-acute care providers have not received a similar subsidy.
Due to these recent pressures, Select Medical Holdings Corporation (“SEM”) released an expected earnings announcement in advance of the actual results, in which it noted “the unpredictable effects of the COVID-19 pandemic, including the duration and extent of disruption on Select Medical’s operations and increases to our labor costs, creates uncertainties about Select Medical’s future operating results and financial condition.”
While we have seen increasing optimism by healthcare providers over the past few quarters, the recent disclosures from the post-acute sector illustrate that the effects of COVID continue to ripple through the healthcare sector. With the fourth quarter results being released over the coming weeks (HCA and Encompass recently released), it will be interesting to hear if other sectors report similar headwinds.
Rising Labor Expense: Potential Impact to 2022 Performance
Healthcare labor expenses continued to exceed historical levels with a 12.6% year-over-year increase based on a recent analysis of over 900 hospitals. Labor expenses grew at a faster rate than the number of clinical hours worked, which supports the notion that rising labor costs were not due to increased staffing levels but rather due to labor shortages driving higher pay to improve employee retention. Part of the labor shortage can be credited to the surge of Delta and Omicron variants in the second half of 2021 that resulted in high volumes of quarantined staff and a reliance on costly contract labor and travel nurses. At the Bank of America December 2021 Home Care Conference, LHC Group announced a decrease in quarantined staff throughout Q4 from a high of 4% down to 1% in December. This indicates that the labor market issues will see some improvement as health systems’ dependence on pandemic-related contract labor declines as COVID-19 surges dissipate going into 2022.
A more concerning challenge faced by all sectors was the shrinking workforce, coined the “Great Resignation.” The Bureau of Labor Statistics reported healthcare and social assistance workers had the second highest quit rate in November 2021 at 6.4% due to increasingly high levels of professional burnout. The waning labor force has prompted companies to offer additional incentives such as shift and retention bonuses. For example, HCA reported during Q3 a 10-12% annual increase in FTEs being in the premium pay categories. Many large public players have voiced an anticipation of continued high levels of premium pay, competitive bases, and higher annual wage inflation to attract and maintain adequate staffing levels in 2022.
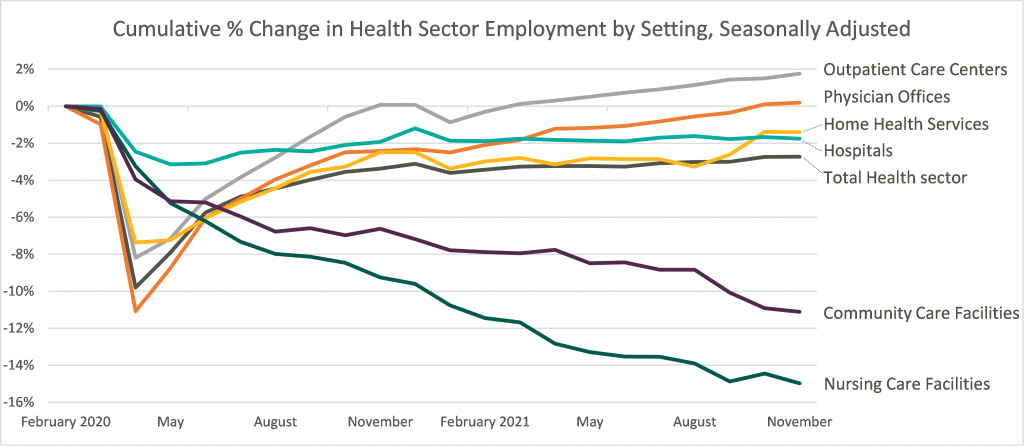
Leaders in the industry have announced initiatives to decrease labor pressure primarily by focusing on recruiting and retention to bounce back to pre-pandemic levels of employment. With a heightened focus on attracting and maintaining adequate levels of hired staff as opposed to contract labor, it appears the overall industry expectation for 2022 is that labor costs will likely decrease compared to 2021 although not to pre-pandemic levels. The chart below shows the percentage change in employment across the healthcare sector from the Bureau of Labor Statistics Job Openings & Labor Turnover Survey from February 2020 to November 2021. This highlights the steady recovery toward pre-pandemic staffing levels for outpatient care and physician offices, the continued employment challenges in home health and hospital settings, and the notable struggle for community and nursing care facilities to return to a state of normalcy.
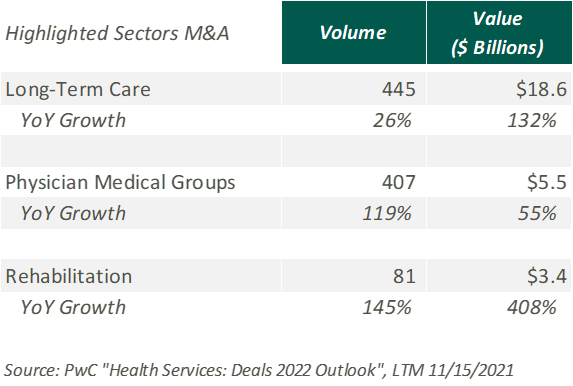
Robust M&A Activity
Deal activity within the healthcare sector was strong in 2021 with industry-specific multiples that reached or in many cases exceeded 2019 levels. Experiencing a noticeable rebound from 2020, volume and value of deals grew by substantial margins on a year-over-year basis. Deal volume in the health services industry rose by 56% while value rose 227% in the TTM 11/15/21 period. Long-term care led all sectors with the highest volume of deals, as seen historically, and continues to remain a hot spot in the transaction space. Similarly, physician medical groups and the rehabilitation sector experienced the largest growth transaction volumes year-over-year.
Physician medical groups have received vast interest in physician employment from private equity firms, new-age value-based care organizations, services arms of managed care giants (Optum, Neue Health), and health systems. This, coupled with independent physician group operating challenges from COVID-19 related volume impact and looming Centers for Medicare and Medicaid Services (CMS) cuts, is creating a robust transaction environment that is expected to continue during 2022. For the rehabilitation sector, strong demographic tailwind, along with the lifted CON moratorium in Florida and continued joint venture interest between health systems and strong rehabilitation operators (Select, Kindred, Encompass), has resulted in material deal volume in the space.
Hospitals and health systems were the only sector to see a decline in volume of deals, down 26% from the previous year. Despite the decline, the total transaction size of deals only dropped slightly year over year, indicating larger deal-size on a per-transaction basis. The acceleration of megadeals taking place, the shifted focus on scale, and the diversification of their business models all drove average total size per deal higher than seen before in 2021.
Price Transparency
Effective January 1, 2021, the Centers for Medicare and Medicaid Services (CMS) implemented a price transparency rule requiring hospitals in the United States to provide accessible pricing information to patients about the cost of the care they may receive. Hospitals must display negotiated rates for all items and services, in a machine-readable format, so that patients can compare prices before arriving at the hospital.
Though, in July 2021, a study was published by PatientsRightsAdvocate.org detailing that a vast majority of hospitals were not compliant with the new rule. At the release of the study, the penalty for non-compliant hospitals was $300 per hospital, per day. While many patients advocate for CMS to stiffen penalties for non-compliant hospitals, healthcare professionals argue against the rule, stating CMS did not provide enough clarity on what the rule should entail.
A vice president of a large U.S. health system discussed the ambiguities around the rule with Fierce Healthcare. “One interpretation is you simply publish your rate schedule – whatever your rate exhibits are in your contracts, publish that and that’s compliant. Another one is to summarize these [CMS] packages [and] what your negotiated charges are.” For many health systems, the resources required to implement their rates in a machine-readable format far outweigh the penalty of remaining non-compliant. The VP stated that he believes many hospitals already provide their rates in a clear, understandable way, but the rule’s lack of clarity and the requirement for a machine-readable format make compliance difficult and costly.
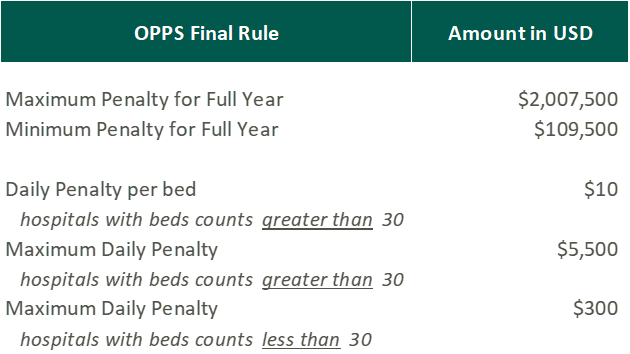
In November 2021, CMS released the 2022 Outpatient Prospective Payment System (OPPS)/Ambulatory Surgery Center (ASC) Payment System final rule (OPPS Final Rule). Within this rule, CMS increased penalties for hospitals that are not compliant with the price transparency rules and removed barriers for patients accessing online pricing information.
While the Final Rule may be beneficial for patients, Stacey Hughes, Executive Vice President for the American Hospital Association (AHA), states that they “are very concerned about the significant increase in penalties for non-compliance with the hospital price transparency rule, particularly in light of the many demands place on hospitals over the past 18 months, including both responding to COVID-19, as well as preparing to implement additional, overlapping price transparency policies.”
The new penalties, visible in the chart above, went into effect on January 1, 2022.
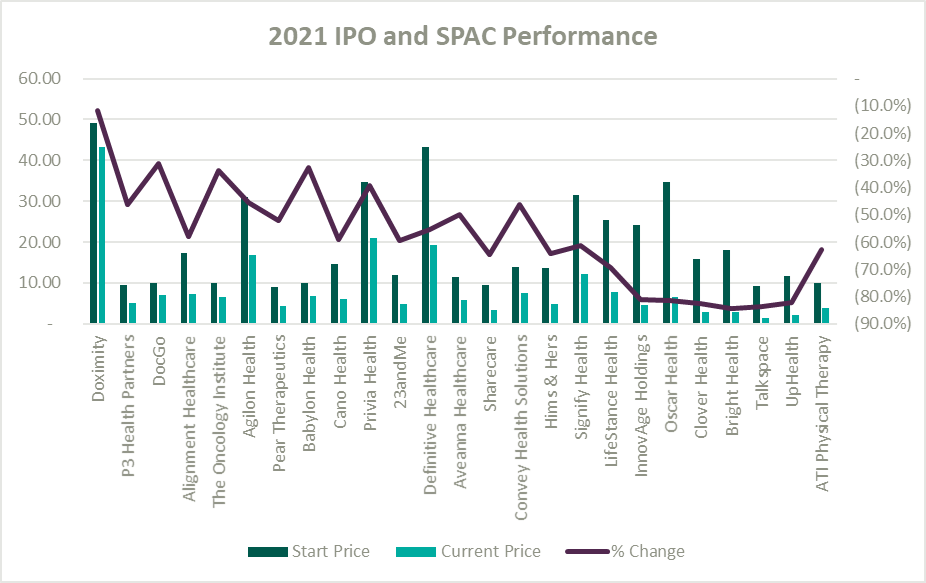
IPO and SPAC Stock Price Performance
A record number of health and health services companies went public during 2021 by way of SPAC or IPO. Rebecca Springer, a private equity analyst with PitchBook noted, “The multiples in public markets are very, very strong right now, so you can get, all else equal, a better return on your investment if you go public with your company rather than selling it to a strategic investor.”
Unfortunately, while the stock market might be performing well, the recently public healthcare operators have not faired as well since their initial offerings. The Healthy Muse Health Tech Index (“HTI”) generally underperformed the overall performance of the stock market, with the majority of the players finishing in red; the HTI declined 35% as opposed to the 27% gain for the S&P 500 during 2021. The public markets seemed like a perfect place for an exit strategy given the multiples observed in the public markets. All recent entrants finished the year below the original IPO price and while the reasons for the price declines varied it is clear the public markets are less forgiving with valuations if an organization does not achieve expectations.
Conclusion
Overall, the healthcare sector experienced highs and lows during 2021 as it continued to navigate a post-COVID world. As pandemic pressures continue into 2022, healthcare institutions will have to keep a close eye on staffing costs and abide by new regulations. Despite these challenges, the appetite for M&A transactions and market participation in the sector remains strong. We look forward to a new year of challenges, wins, and continued changes in this interesting industry.
By: Jordan Tussy, Hunter Hamilton and William Teague, CFA
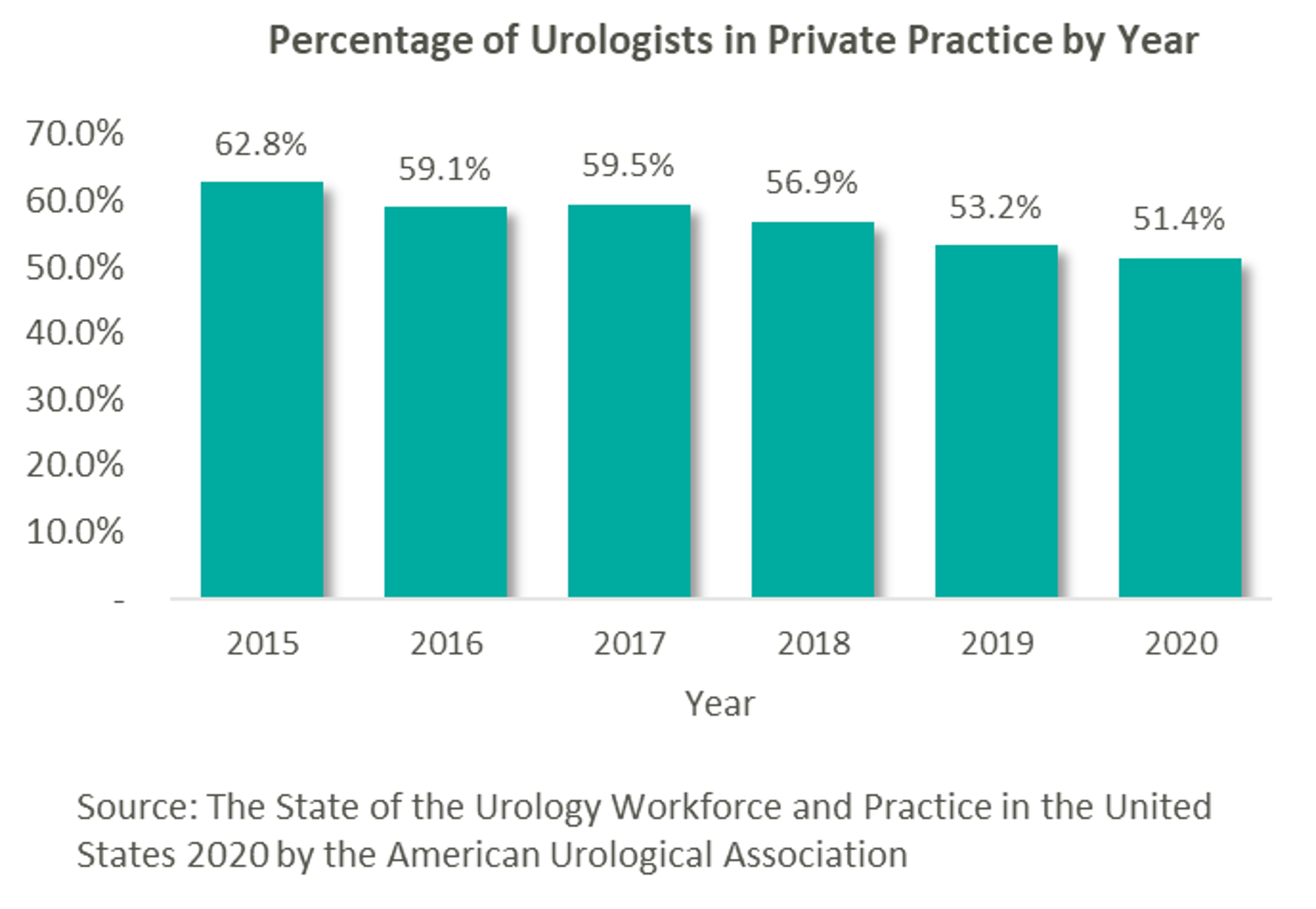
As many physician specialties begin to mature (e.g., gastroenterology, dermatology and ophthalmology), funds have started to flow into the urology space from private equity (“PE”) firms still eyeing platform acquisitions. “Competition for quality assets in this segment is still pretty light. There are a number of independent urology groups of scale with good management teams and back-office infrastructure,” stated Jeanne Proia of Cross Keys Capital in an interview with Mergermarket. [1] Growth prospects for urology practices are also particularly strong due to increases in life expectancy that have led to increases in demand for urologic services. Additionally, an expected shortage of urologists estimated to exceed 3,600 by 2025 will only further amplify the situation. [2] Urology’s several sources of ancillary revenue such as lab & pathology services, lithotripsy, radiation oncology, and ambulatory surgery make the specialty particularly attractive to platforms seeking to execute a roll-up strategy. With over 13,000 urology providers, 51.4% of whom work in private practice, this fragmented market offers PE firms the opportunity to facilitate consolidation. [3]
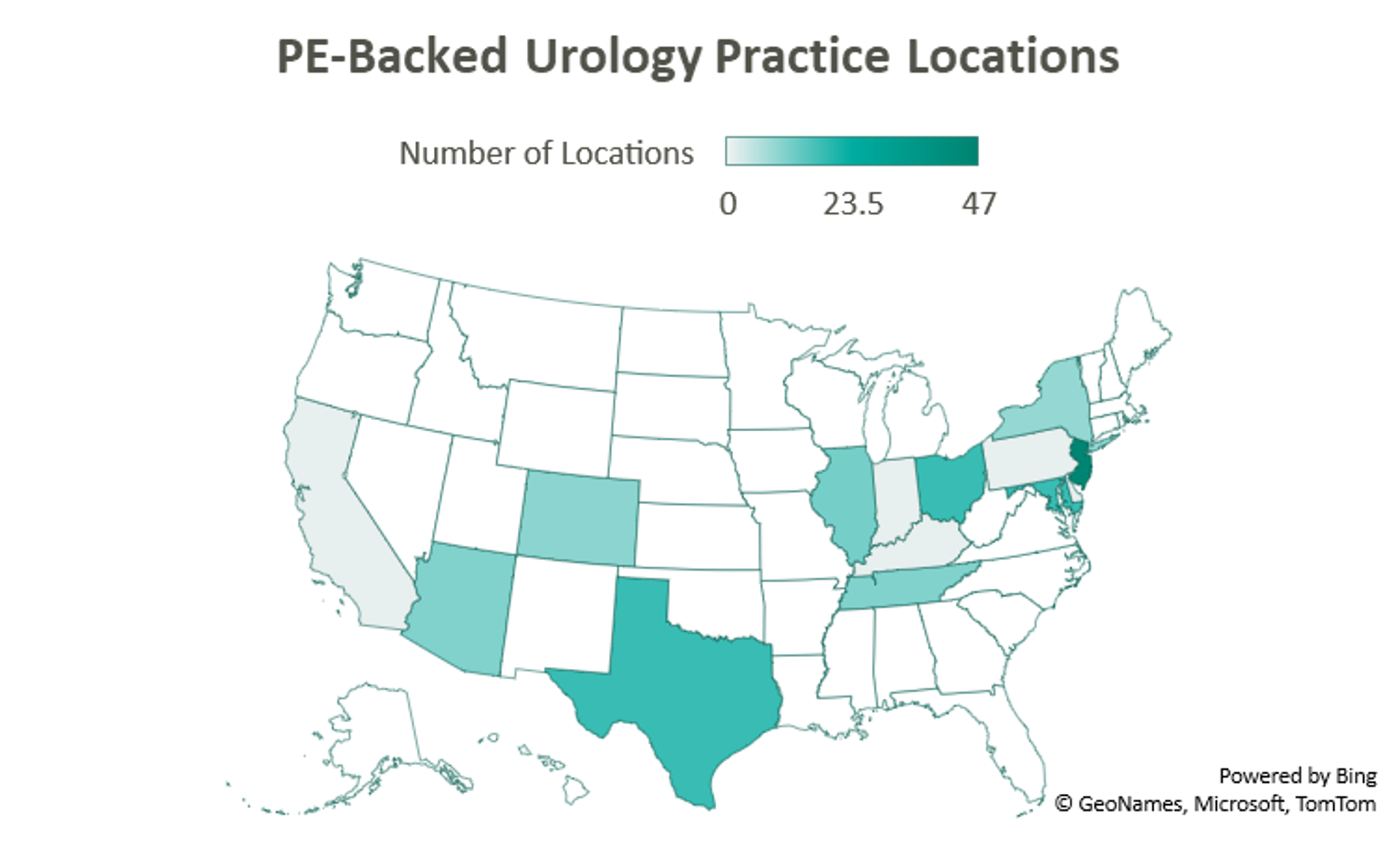
This prospect, paired with the strong demand for urologic services, has led to significant investment interest in the space, which can trace its roots back to August 2016 with Audax Private Equity’s partnership with Chesapeake Urology and the resulting formation of United Urology Group (“UUG”).
United Urology Group
Since acquiring Maryland’s Chesapeake Urology, Audax Private Equity’s UUG has further expanded its footprint both locally in Maryland, as well as nationally. Most recently, UUG has entered Arizona markets through its partnership with Arizona Urology Specialists in late 2019 and additional affiliations with Arizona Institute of Urology and Urological Associates of Southern Arizona in January of this year. Through this most recent partnership, UUG now operates out of 25 offices in Delaware and Maryland, 11 facilities in Tennessee, 10 offices in Colorado, and 23 locations in Arizona. With these locations and over 220 physicians, UUG remains committed to providing accessible care. [4]
Urology Management Associates
Prospect Hill Growth Partners (formerly known as J.W. Childs Associates) partnered with New Jersey Urology (“NJU”), a practice comprised of 96 providers in 46 New Jersey locations, to form Urology Management Associates (“UMA”) in September 2018. [5] NJU, having previously merged with Delaware Valley Urology in April 2018, represented the largest group of urologists in the United States at the time. Since then, UMA has expanded through a partnership with Premier Urology Group in September 2019 and Urology Care Alliance in December 2019. This latest affiliation expanded the platform’s presence in New Jersey and established its stake in Pennsylvania. UMA currently has over 150 providers and operates out of 64 locations, including 6 cancer treatment centers. [6]
U.S. Urology Partners
A 2018 strategic investment by NMS Capital in Central Ohio Urology Group launched US Urology Partners as an employment alternative for practices wanting to maintain their independence. As of August 2019, the hope of the organization’s CEO Mark Cherney was to grow US Urology Partners’ roughly $50M in revenue 10x in the next 3-5 years. Cherney also indicated that urology may be the next physician specialty to see significant consolidation, stating that “while the other physician specialties such as dermatology, dental and ophthalmology have seen heavy M&A activity in recent years, urology has remained relatively untapped for sponsor investment.” [7] Cherney cites shrinking rates of reimbursement, growing administrative costs, a complex regulatory environment, and a lack of independence as deterrents to hospital employment, while a national platform partnership on the other hand can provide “greater management support and financial strength.” [8] The group most recently partnered with Associated Medical Professionals of New York, a nearly 30-physician practice operating out of 9 locations throughout the Central New York region. Ancillary services offered by the practice include radiation oncology, pathology, imaging, lithotripsy services, as well as clinical research. [9]
Solaris Health
Another big presence in the space is Lee Equity Partners, who in June 2020 acquired and merged Integrated Medical Professionals and The Urology Group to form Solaris Health. The goal of Solaris “is to build a national platform that attracts leading independent urological partners who are committed to providing quality and value in healthcare.” [10] The platform has since expanded from its origins in New York, Ohio, Kentucky, and Indiana into Pennsylvania through a partnership with MidLantic Urology and, most recently, into Illinois through an affiliation with Chicago’s Associated Urological Specialists in March of this year. With more than 262 providers, Solaris now operates out of more than 11 sites in six states. [11]
Urology America
With its formal acquisition of Texas-based Urology Austin in October 2020, Gauge Capital established Urology America, a fully integrated urology network providing comprehensive urologic care. The largest urology practice in the metro Austin area, Urology Austin brought 18 locations and over 50 providers to the platform. Also included in the transaction were Urology Austin’s clinical research department, patient navigation programs, pelvic floor physical therapy, the Austin Center for Radiation Oncology, as well as a nationally accredited in-house pharmacy and pathology laboratory. Urology America is currently seeking to partner with urology practices nationally recognized as innovators and leaders in the field. [12]
Urology Partners of America
New to the space is Triton Pacific Capital Partners. This May, the Los Angeles private equity firm partnered with Genesis Healthcare Partners (“GHP”), a Southern California urology group with 48 providers and 15 locations, to establish Urology Partners of America (“UPA”). At the time of the transaction, GHP represented the largest independent urology group on the West Coast. With a current focus on further expansion across the Western States, the platform has a long-term goal, according to UPA CEO, Marshal Salomon, of building “the business to 200+ physicians within the next few years.” [13]
Future of the Field
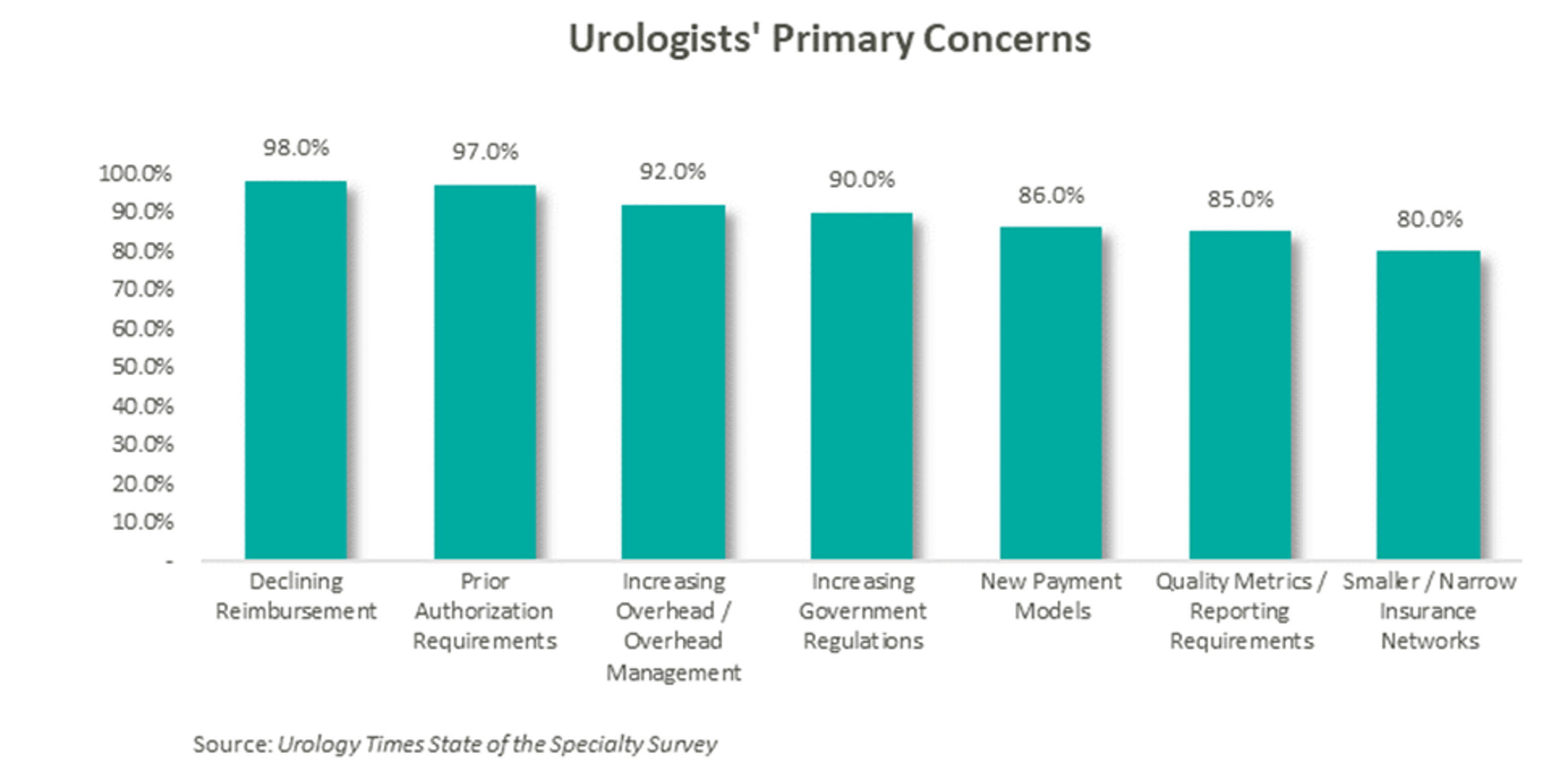
According to data compiled by Urology Times, over 90% of urologists surveyed are concerned about declining reimbursement trends, growing regulation, and increasing overhead costs. [14] Furthermore, a study published in the July 2021 Issue of The Journal of Urology revealed that the average rate of reimbursement per urologic procedure decreased by an average of 0.4% per year from 2000 to 2020 before adjusting for inflation. [15]
As a result of these pressures, independent physicians are seeking alternative employment structures to private practice. PE firms are an attractive option due to their ability to alleviate some of the administrative burden, strengthen payor negotiations though scale, provide access to additional capital and allow the providers to focus on their clinical services. With this model, physicians receive upfront compensation from the acquisition and may retain an equity position in the new entity. They often agree to a reduction in their historical compensation as a trade-off for the promise of future equity returns and current liquidity. The success of the model depends on the ability of the PE firm to provide both operational and financial value to the practice and deliver on earnings repair. Otherwise, shareholder physicians may not continue to perform at historical levels, and non-shareholder physicians may begin to reconsider private practice.
Since the formation of United Urology Group, there has been a trend of PE-backed urology practice consolidation over the past 5 years. Given that most urology visits are with patients over the age of 65 and that nearly 20% of the population is expected to be 65 or older by 2030, demand for urologic services is only expected to increase. [16] With increasing demand, fragmentation, and a complex regulatory environment, continued consolidation should be expected in the urology space. The ability to deliver on earnings recapture through the successful implementation of economies of scale will ultimately determine the outcome of these platforms, as the value of the model hinges on the loyalty of the urologists.
Now Trending in Behavioral Health: Integration Strategy, Regulatory Compliance, & Transactions
August 10, 2021
At the American Health Law Association’s 2021 Annual Meeting, held in June, VMG Health Managing Director Clinton Flume, presented trends within the behavioral health industry, along with co-presenter Jenna Gunville of the law firm Polsinelli. The excerpt highlights Mr. Flume’s observations of the continued consolidation within the behavioral health industry.
Can you talk about the fluctuations in market transactions over the last few years?
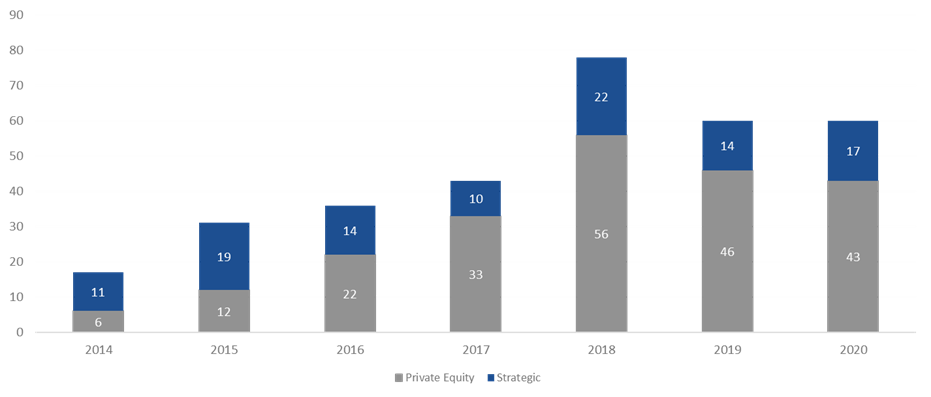
Behavioral health has been a very active market over the last three to four years. 2018 was the high-water mark, with over 75 transactions. 2019 fell off a bit as owners and operators integrated these transactions within their platforms. Obviously, COVID-19 hit 2020, but the year started off well. As year-end numbers became available at the beginning of 2021, the industry anticipated total transaction numbers to be a bit soft but was pleasantly surprised that the deal count came in roughly the same as 2019. This boded very well for continued transaction acceleration in 2021, which is on pace to surpass 2019.
2014–2020 Total Behavioral Health Acquisitions [1]
What factors are key contributors to the increase in behavioral health transactions?
The Global Behavioral Health Market is expected to garner growth at a compounded annual growth rate of 5.0% from 2020 to 2027 and to reach a value of around $242 billion by 2027[2]. The two main factors that I believe will continue to help spur activity are public perception and acceptance and continued investment by private equity. Perception and acceptance involve the acknowledgement and social understanding that mental health services are just as important as the physical treatments we receive as a collective. High profile government official and celebrities certainly aid in bringing awareness to and lessening the social stigma around mental health struggles.
In addition, I believe that payor parity and investment in platform digital health services are key contributors to the increase in transactions. Payor parity focuses on the historical noncompliance of insurers in reimbursing providers for mental health services and creating equal footing for reimbursement and access to services. Increased legislative scrutiny and enforcement of health plans and reimbursement expansion though the Coronavirus Preparedness and Response Supplemental Appropriations Act are two ways payor parity has recently been addressed.
Can you comment on the sub-industry transactions mix and tell us how this mix may impact future consolidation of behavioral health?
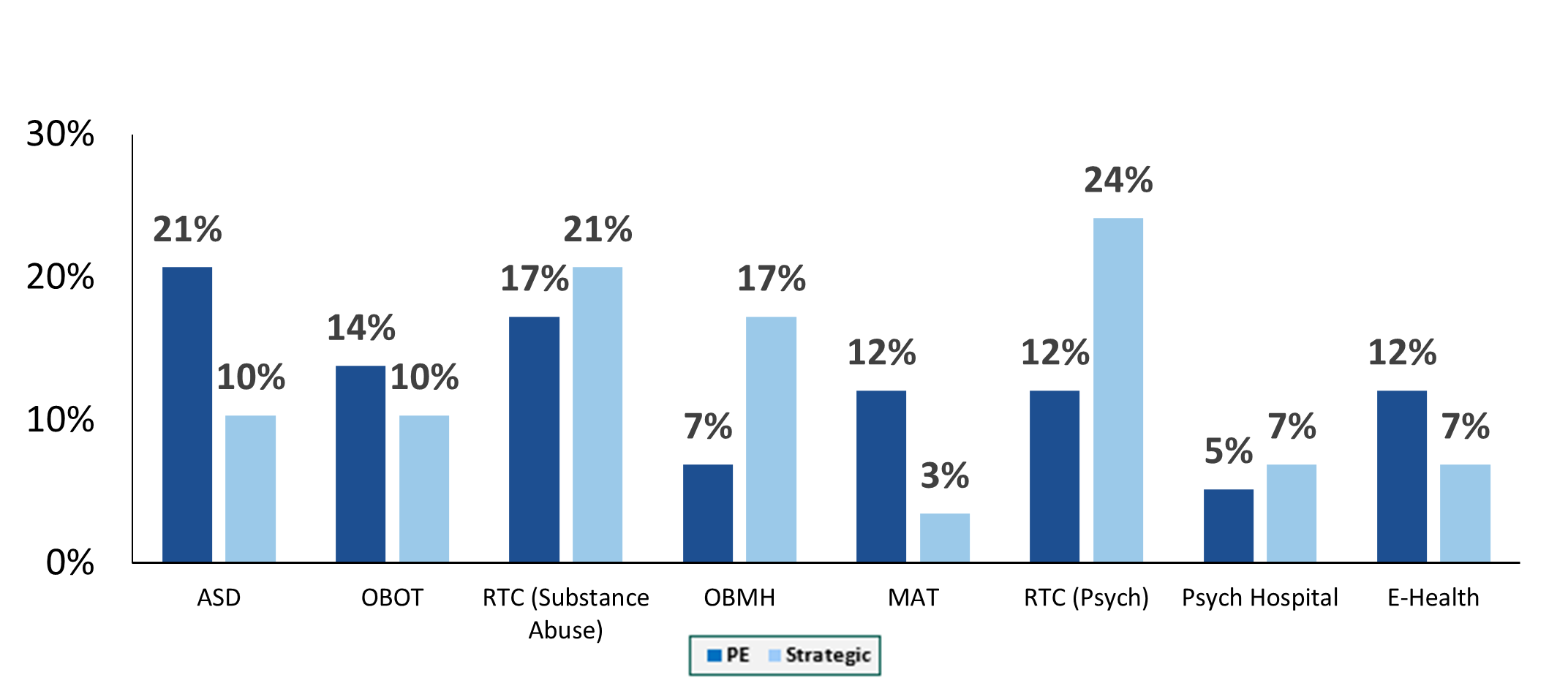
Autism spectrum disorder transactions have exhibited the greatest share of transaction growth since 2018. This is largely driven by acknowledgement of an underserved industry, legislation that includes the Autism CARES Act of 2019, and improvements in reimbursement. Residential treatment centers (both substance abuse and mental health), along with office-based treatment facilities, continue to occupy the bulk of transactions. One area we have been seeing real growth in over the last two years is digital health transactions. These deals include digital technology administration of services such as direct-to-consumer care, revenue cycle performance improvement and automation, and artificial intelligence applications for managing and treating substance abuse and mental health disorders. In June, Rock Health[3] stated that U.S. behavioral health digital startup companies raised $588 million in the first half 0f 2021, which is equal to the annual amount this segment received in funding for any prior year. As we look at 2021 and beyond, we expect that digital health platforms and direct-to-consumer technology will accelerate the growth and acceptance of mental health services.
2020 Percentage of Acquisitions Involving One or Multiple Service Lines [4]
Sources:
[1] The merger and acquisition data contained in various charts and tables in this report has been included only with permission of the publisher of Deal Search Online, HealthCareMandA.com. All rights reserved.
[4] The merger and acquisition data contained in various charts and tables in this report has been included only with permission of the publisher of Deal Search Online, HealthCareMandA.com. All rights reserved.
Oncology: Private Equity Investment in Cancer Care
July 27, 2021
By: Vince Kickirillo, Jordan Tussy & Hunter Hamilton
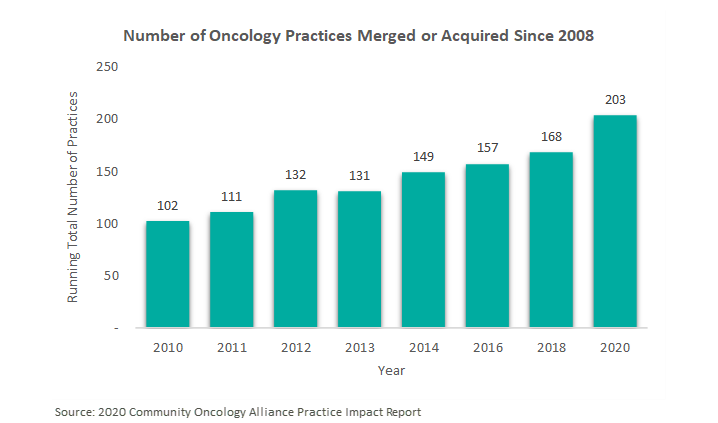
In August 2019, VMG Health published an article titled “Oncology on the Rise: Private Equity Investment in Cancer Care.” This article discussed the emerging interest in the oncology provider industry by private equity (“PE”) firms, most notably through the formation of PE-backed platform practices. Since this article was published, the oncology practices have continued to trend toward consolidation. According to the 2020 Community Oncology Alliance Practice Impact Report, the number of community oncology practices merging or being acquired by another practice or corporate entity, such as a private equity firm, has increased almost 21% since 2018. In fact, trends over the previous ten years suggest there has been an approximately 7.0% annual increase, on average, in the number of community oncology practices that have been acquired by a corporate entity and/or merged with another oncology practice. [1]
However, more recent deal activity suggests a shift from the large-scale platform transactions to tuck-in acquisitions by these platform entities as they seek to scale their businesses in both geography and size.
Tuck-in Acquisitions
As previously mentioned, there has been an uptick in tuck-in acquisitions in the oncology space following the emergence of these PE-backed platforms throughout 2018. These platforms strategically target practices for consolidation to leverage geographic expansion, economies of scale, or hospital affiliations. Below is a summary of the recent activity of the major PE-backed oncology platforms.
Alliance Health Services
Following its acquisition by Tahoe Investment Group in April 2017, Alliance Healthcare Services has continued its national oncology and radiology platform expansion through direct partnerships with physicians and hospitals, such as Beaufort Memorial Hospital in South Carolina and SCL Health in Colorado. “Across the US, we work side by side with more than a thousand hospitals to deliver effective and efficient diagnostic radiology, radiation therapy and related services. We believe it is the best of both worlds: a focus on each unique community, partnership and patients, supported by national resources,” said Rhonda Longmore-Grund, President and CEO of Alliance HealthCare Services. [2]
On June 25, 2021, Alliance announced its acquisition by Akumin for $820 million, which is expected to close in Q3 2021. After holding the platform for 5 years, Tahoe Investment Group will transition to a minority ownership position in the publicly traded, combined entity. Regarding the transaction, Riadh Zine, President and CEO of Akumin, stated “The acquisition of Alliance is transformative in a changing healthcare ecosystem that continues to shift toward outpatient, price-transparent, value-based care. There’s no other organization that has the complement of attributes we will offer together as outpatient healthcare services experts, in particular with Alliance’s longstanding hospital and health system relationships and Akumin’s freestanding operational expertise.” The combined company is projected to have pro forma revenue in excess of $730 million and EBITDA of approximately $210 million based on the trailing twelve months ended March 31, 2021. [3]
Verdi Oncology
Founded in 2018 with the acquisition of Horizon Oncology by Pharos Capital Group, Verdi Oncology has since expanded into the Tennessee and Texas Markets. In July 2019, Verdi announced a partnership with Nashville Oncology Associates, a two-physician medical oncology practice, in which the platform would provide management services, economies of scale, and infrastructure.[4] Similarly, in August 2019, the company launched Verdi Cancer and Research Center of Texas, which would provide medical oncology services and early phase clinical trials in Dallas-Fort Worth. [5]
OneOncology
Since its founding in 2018 by General Atlantic, OneOncology has continued to expand its physician network in both size and geography. The platform, now comprised of 600 providers at 189 sites, has acquired, and subsequently grown, practices in Arizona, California, New England, Pennsylvania, New Jersey, and Texas. [6] For example, OneOncology partnered with North Texas-based Center for Cancer and Blood Disorders (“CCBD”) in 2020 and recently announced the addition of three practices and fourteen physicians to the Texas affiliate. [7] OneOncology targets leading community oncology practices to provide comprehensive and cost-effective cancer care. Oncologists are attracted to the platform’s business model which allows them to remain independent while expanding their services and offering advanced treatment options. “OneOncology gives us the best path forward to continue to bring our patients in Central Pennsylvania advanced cancer care and to grow our clinical trial program. Working with other leading oncology practices across the country who share our vision for delivering the highest quality care in the community setting is what sets OneOncology apart” said Satish Shah, MD of Gettysburg Cancer Center, one of the platform’s most recent targets. [8]
Integrated Oncology Network
Silver Oak Services Partners led the recapitalization of Integrated Oncology Network (“ION”) in October 2018. Shortly thereafter, ION continued its growth strategy with the 2019 acquisitions of Gamma West Cancer Services (“Gamma West”) and e+CancerCare. As a result of the e+CancerCare acquisition from Kohlberg & Company, ION added 21 outpatient cancer care centers in 10 states. [9] Similarly, the platform expanded their services into communities in Utah, Nevada, Wyoming, and Idaho with the Gamma West acquisition. [10] This partnership also advanced ION’s strategy to affiliate with quality healthcare systems. Recently, ION created a new multispecialty platform in the Cleveland, Ohio market with the acquisition of Southwest Urology in January 2021. As stated by Josh Johnson, ION CEO, “This new venture with Southwest Urology represents a pivotal moment in ION’s strategic direction. Our entrance into the urology space with such a highly-respected practice strengthens our capabilities and positions ION to continue growing specialty networks across the country.” [11]
21st Century Oncology
KKR-backed GenesisCare, an Australian oncology platform, acquired previous standalone operator, 21st Century Oncology. The transaction was completed in May 2020 and valued at over $1 billion. At the time, 21st Century Oncology operated out of 293 locations with nearly 900 affiliate physicians in 15 states. [12] Now the combined entity collectively operates with over 5,000 physicians at 440 locations across the world. [13]
Corporate-Backed, Standalone & Other Operators
Updating our August 2019 article, the following section addresses follow-up items on previously discussed corporate-backed and standalone operators, McKesson’s The US Oncology Network and Cancer Treatment Centers of America, as well as two new operators, American Oncology Network and The Oncology Institute.
The US Oncology Network
Since July 2019, The US Oncology Network has expanded its presence in California, Pennsylvania, Indiana, and Texas through partnerships with Northern California Prostate Cancer Center, Alliance Cancer Specialists, Northwest Oncology, and Texas Colon & Rectal Specialists. Since April 2020, the Network has brought over 131 new physicians into the organization.[14]
Cancer Treatment Centers of America
Cancer Treatment Centers of America, an owner and operator of cancer care hospitals and outpatient care centers, announced in November 2020 a partnership with Miller County Hospital designed to meet cancer care needs of Southwest Georgia residents. The organization also notably sold CTCA Philadelphia to Temple University Hospital and announced the closure of CTCA Tulsa in March of this year. CTCA Atlanta opened a comprehensive Women’s Cancer Center this past June with 8 physicians.[15]
American Oncology Network
Though not currently backed by a private equity group, American Oncology Network (“AON”) has gained significant ground in the oncology space over the past few years. Since its founding in mid-2018, AON, a nationwide group of physician practices focused on improving outcomes in community-based oncology, has expanded to include over 170 providers across 17 states. New partnerships in the past year have been forged in Michigan, Georgia, Washington, Arizona, and Maryland. They also have a presence in Idaho with the recent addition of Summit Cancer Centers.[16] According to recent press releases, reasons given for aligning with AON include greater access to resources (i.e., outpatient pharmacy, pathology, and laboratory services), enhanced care management and technological capabilities. Most recently, AON finalized an $85 million financing package with PNC Bank, priming the organization for continued growth in the development of its information technology platforms, pharmaceutical purchases, practice acquisitions, and expansion of service-line offerings.[17]
The Oncology Institute
Another sub-sector within the oncology space that has garnered recent interest is value-based care. Recently, DFP Healthcare Acquisitions Corp (“DFP”), a special purpose acquisition company (“SPAC”) announced the acquisition of The Oncology Institute (“TOI”), a market-leader in providing value-based oncology care. Regarding the transaction, Richard Barasch, one of the sponsors of DFP, stated “[TOI] has created a scalable, replicable model with difficult-to-duplicate capabilities that facilitate rapid expansion… this business combination will create a well-capitalized company that is poised to expand organically, through accretive M&A activity, and via strategic payor relationships.” While TOI currently operates 50 community-based practices in Florida, Arizona, Nevada, and California, they plan to pursue organic growth opportunities and strategic acquisitions in both new and existing markets.[18]
Future of the Field
While the oncology industry continues to trend toward consolidation, there has been a shift from the acquisition or establishment of platform practices to the acquisition of tuck-ins as existing platforms focus on growth through strategic partnerships with practices and physicians. Even with the emergence of such platforms and their subsequent tuck-in activity, the oncology market remains fragmented and poised for continued consolidation as physicians seek alternatives to hospital employment.
Furthermore, private equity firms hold their investments for an average of three to seven years. This trend can be evidenced by the recently announced acquisition of Alliance Healthcare Services by Akumin after five years of ownership by Tahoe Investment Group. Given the age of several of the other platforms, it is likely there will be recapitalizations of these businesses over the next few years.
Post-COVID Hospital Guidance: Comparing Full-Year Guidance from Public Hospital Operators before the COVID-19 Pandemic and One-Year Later
June 9, 2021
Last March, the United States declared a national emergency related to the coronavirus (“COVID-19”) pandemic. At the time and throughout the beginning of the pandemic, meaningful economic factors were unknown including the evolution of the disease, the extent of its economic impact, and the results of steps taken and yet to be taken by the federal government, financial institutions, and market participants. As a result, many healthcare operators suspended the disclosure of earnings guidance. Now, after a year of experience with the COVID-19 pandemic, operators have resumed sharing their expectations of future financial performance. VMG Health analyzed select guidance figures from the four main public hospital operators to better understand the industry’s perspective on operations in a post-COVID world.
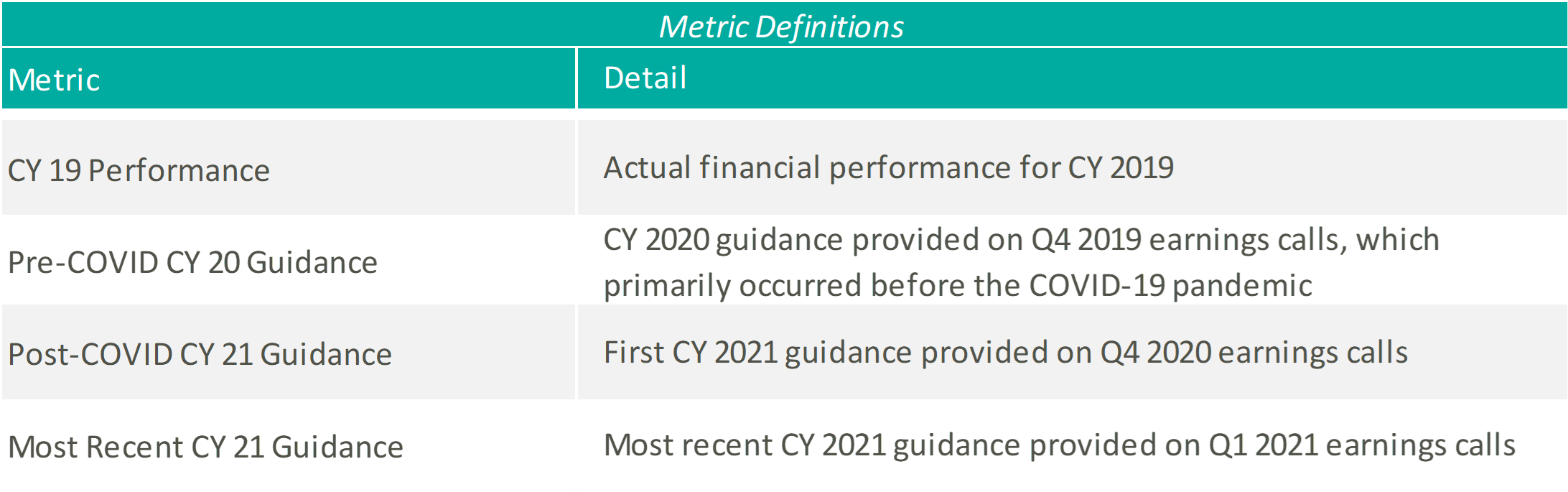
Please see below for a list of the public hospital operators examined, as well as further detail regarding the various metrics considered.
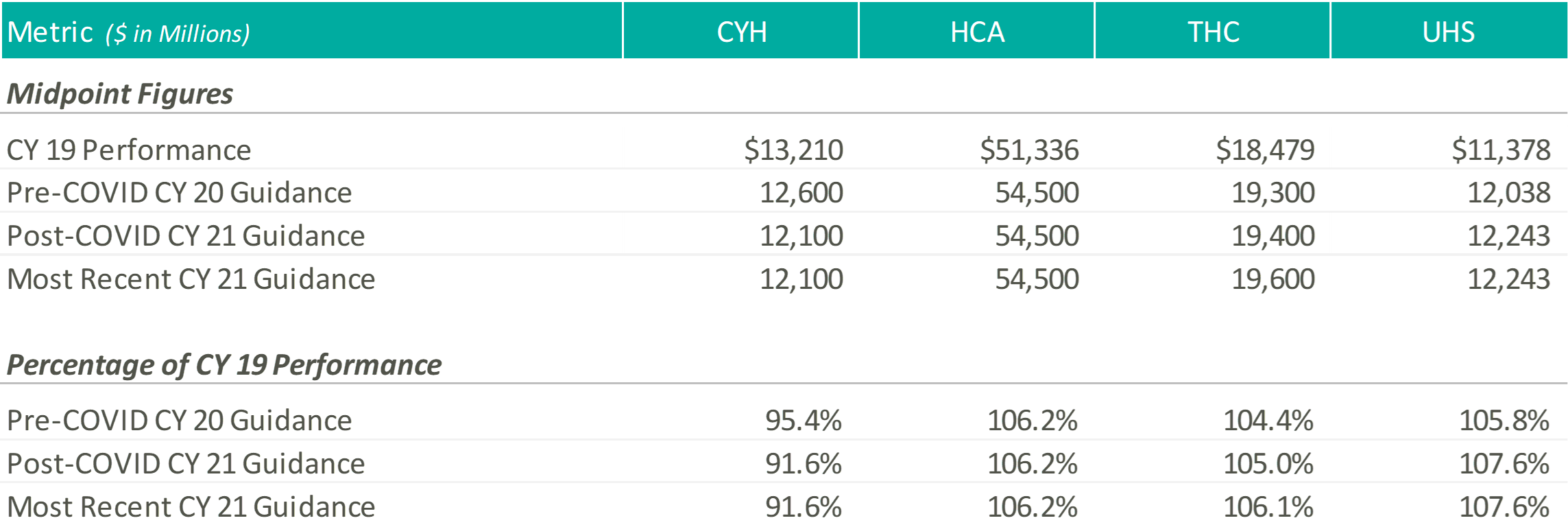
Revenue
Except for CYH, initially and most recently, the hospital operators expect CY 2021 revenue levels at or above those estimated at the beginning of CY 2020, and well above their CY 2019 performance. Please note, CYH completed a planned divestiture program towards the end of 2020, making it difficult to compare CY 2019 performance to the forward guidance figures.
At the end of 2020, when the hospital operators were once again comfortable providing guidance figures, the management teams anticipated continued COVID volumes during the first half of the year, with a return to more normal levels by the second half of the year. HCA noted that they expected 2021 volumes to grow above 2020 levels but trend slightly below 2019 levels, while THC believed their 2021 volumes would improve on 2019.
A few months later, during the Q1 2021 earnings calls, the operators noted strong first quarter results and tailwinds from the extension of sequestration through the end of the year. As a result, HCA tightened their CY 2021 revenue guidance and THC increased their CY 2021 revenue guidance. Although UHS kept their CY 2021 guidance figures flat, they noted that they “remained comfortable” in their ability to achieve the projected revenue levels and viewed sequestration as a “cushion” not currently factored into their guidance figures.
Adjusted EBITDA
Except for UHS, initially and most recently, the hospital operators expect CY 2021 adjusted EBITDA levels near or above those estimated at the beginning of CY 2020 and their CY 2019 performance.
As mentioned previously, the operators pointed towards a strong first quarter performance as rationale for tightening or raising their CY 2021 EBITDA guidance ranges. Additionally, HCA, CHS, and THC discussed the continued focus on cost saving initiatives throughout 2021 to combat expense pressures related to the COVID-19 pandemic.
During the Q4 2020 and Q1 2021 earnings calls, UHS management cited similar expense pressures, primarily related to labor, associated with the COVID-19 pandemic. Generally, the UHS team expects the labor pressures to ease as the volume of COVID patients declines, but at a slower pace.
CONCLUSION
Although uncertainty remains, with a full year of COVID-19 operations under their belts, hospital operators have become more comfortable discussing go-forward performance. As Daniel Cancelmi, CFO and Executive VP at THC said during the Q4 2020 earnings call, “Although there are various uncertainties as to how the pandemic will impact us this year, we believe we have sufficient visibility and confidence as to how our business will perform during the ebbs and flows of the pandemic to enable us to provide investors an outlook of our projected results this year.” Additionally, Kevin Hammons, Executive VP and CFO at CYH, noted that although uncertainty remains, there are multiple ways to achieve the guidance figures. After a hard year for the healthcare industry, it is encouraging to see the hospital operators look forward again and provide a generally positive outlook related to the recovery from the COVID-19 pandemic.
The future of the 340B Program remains up in the air as policy makers continue to scrutinize its reimbursement model, citing a potential contribution to rising drug costs and a shift in site-of-service for cancer treatment.8,20 Will the uncertainty of 340B disincentivize hospital consolidation of oncology practices? Is this Program contributing to the shift in oncology treatment from free-standing clinics to hospital outpatient facilities? Many are asking what the future holds for the 340B Program and what the repercussions will be if significant changes are implemented.
340B Program Overview
The 340B Program requires drug manufacturers to offer qualified healthcare providers substantial discounts on select outpatient drugs. The formula used to calculate the “ceiling price”, or the maximum price a manufacturer can charge for a 340B drug, is based on the Medicaid drug rebate formula. It is the average manufacturer price (“AMP”) less a unit rebate amount (“URA”), which is specified in the Social Security Act (“SSA”) and varies by type of drug.21 Generally, the six hospital categories listed below can qualify as a “covered entity” and be eligible for the Program.
Disproportionate share hospitals (DSHs);
Children’s hospitals;
Cancer hospitals (those exempt from Medicare);
Sole community hospitals;
Rural referral centers; and,
Critical access hospitals.
The 340B Program was founded in 1992 with the goal of reducing drug costs for the listed entities and enhance access to prescription medication to vulnerable patients.
In 2010, the 340B Program experienced significant expansion with the passage of the Patient Protection and Affordable Care Act (“PPACA”).9 However, in recent years, CMS has enacted several budget cuts targeting the 340B Program and its reimbursement for drug costs, leaving the Program’s future in question. More cuts and/or structural changes to the 340B Program should be expected, as lawmakers re-evaluate the effectiveness of the current payment model.
340B Program Key Milestones
Some of the key dates in the history of the 340B Program are outlined chronologically below.
1992: 340B Program Enacted
Section 340B of the Public Health Service Act was enacted by Congress. Manufacturers of pharmaceutical drugs were required to enter into a pharmaceutical pricing agreement (“PPA”). The PPA agreement required manufacturers to provide front-end discounts to “covered entities”. Discounts are applied to qualified outpatient drugs to covered entities that serve the most at-risk populations.4
2018: CMS Final Rule
CMS final rule pays 340B hospitals 77.5% of the average sale price (“ASP”) for most Part B drugs. This payment rate was determined based on an analysis in 2015 the MedPAC report, which indicated the average discount received on 340B covered drugs was 22.5%.21 CMS historically paid 106.0% of the ASP.1
In December 2018, a Federal Judge from the US District Court for the District of Columbia ruled that CMS did not have the authority to change the payment rates because it had not collected enough data on the hospitals’ acquisition costs to justify the payment cuts.3, 6 HHS has appealed the ruling and continued to reimburse 340B hospitals at ASP minus 22.5%.6
November 2019: Proceed with Reimbursement Cuts
CMS announces plans to move forward with reimbursement cuts to 340B safety-net hospitals in 2020 despite pending litigation.11
January 2020: Hospital Eligibility Called into Question
The US Government Accountability Office (“GAO”) published the results of a study on the HRSA oversight of non-government 340B hospitals, which found the current processes did not provide adequate assurance that hospitals were meeting eligibility requirements for 340B participation. As a result, GAO recommended six steps for the HRSA to implement to improve these processes. The results of this study support the notion that 340B hospitals may face greater scrutiny in the future.12
March 2020: Program Incentives Not Aligned
Some have claimed that the 340B Program may incentivize qualifying hospitals to use more expensive cancer drugs. However, a study in the March MedPAC report to Congress concluded that there was little evidence to support the idea that 340B status influences cancer spending.13
April 2020: Approval of Hospital Survey
In response to the federal ruling, CMS received approval to survey 340B hospitals to collect drug acquisition costs2. The collected data may be used to determine future reimbursement rates for drugs purchased under the 340B Program. The goal, as stated by the agency, is “to ensure that the Medicare Program pays for specified covered outpatient drugs purchased under the 340B Program at amounts that approximate what hospitals actually pay to acquire the drugs.”3 Hospitals were required to submit the surveys by May 15th.7
July 2020: Trump Administration Announces Drug Price Cuts
President Trump signed four executive orders that will ultimately lower costs on prescription drugs, including insulin and epinephrine. Hospitals who purchase insulins and epinephrine through the 340B Program must pass the savings from discounted drug prices directly to the underserved patient.17
July 2020: U.S. Court of Appeals Upholds CMS Payment Cuts
On July 31, 2020, the U.S. Court of Appeals reversed a previous ruling, which claimed CMS did not have authority to change payment rates for the 340B drug discount Program. As a result, the 28.5% cuts to part B drug reimbursement for 340B hospitals are permitted to continue.18
August 2020: CMS Proposed Rule
On August 4th, CMS released the OPPS/ASC Payment System proposed rule for CY 2021, which included new proposed rates for covered 340B drugs based on results of the hospital survey. While CMS has proposed adopting rates of ASP minus 28.7% for 340B-acquired drugs, they have also solicited comment on continuing payments of ASP minus 22.5% instead. Additionally, CMS has proposed that children’s hospitals, rural sole community hospitals, and PPS-exempt cancer hospitals be exempt from either of the proposed policies and continue to be paid ASP plus 6%.19
How might changes to the 340B Program affect Oncology M&A?
As indicated in the March 2020 MedPAC report to Congress, cancer drugs from hospital outpatient departments comprise approximately 73% of total Medicare Part B drug spending. Consequently, any sustained budget cuts to the 340B Program would likely have significant effects on the oncology sector. For instance, a report by the community oncology alliance states “the 340B Pricing Program has fueled significant consolidation of the nation’s cancer care system, driving independent, community oncology practices to close or merge with hospital outpatient departments.” If CMS proceeds with the 340B reimbursement cuts, will hospitals become less incentivized to acquire oncology practices?
While changes to the 340B Program may create a major headwind for the oncology industry, the overall demographics for cancer treatment in America remain strong enough to spur attractive investment consideration. According to the American Cancer Society, approximately 80% of new cancer diagnoses occur in individuals aged 55 years and older.14 Given the current population trajectory, which projects approximately 20% of the population will be over the age of 65 by 203015, it is estimated that the incidence of cancer will continue to increase, from approximately 17.0 million in 2018 to 26.0 million in 2040.16 These factors will likely result in an increase in demand for oncology providers and services over the next ten years.
This notion is supported by the recent uptick in investment activity in the oncology provider space. In June 2019, e+CancerCare was acquired by the private equity group, Silver Oak, and then combined into larger Integrated Oncology Network. Additionally, Genesiscare acquired 21st Century Oncology on May 15, 2020.22 This recent activity suggests that even with the uncertainty, the oncology space remains ripe for investment.
The mixed trends facing the oncology sector suggests that hospitals and other potential acquirers will need to perform careful and proper due diligence to determine whether making investments in the oncology space is appropriate for their organization. With looming regulation on the horizon, it remains to be seen whether oncology practices continue to consolidate into hospitals, pursue alternative investment strategies in private equity firms or practice management groups, or revert to independent status.