
Written by David Lamonte, CFA
The finalized Radiation Oncology payment model and the Final CY 2021 Medicare Physician Fee Schedule (“MPFS”) have now been made public. Many in the industry will continue to face downward pressure on reimbursement during the coming year under the new MPFS payment rates set by Medicare which will drive overall cuts estimated to average 5.0% for all Medicare revenues.
Many in the industry have indicated the effect of these cuts could result in less availability of treatment options to patients as those providers at the margins experience further pressure on profitability. Block Lease Arrangements are one form of loose consolidation among providers which can offer a solution to the contracting reimbursement and rising costs seen by many. A block lease is formed when a provider leases certain services or assets for a defined “block” of time to the lessee who retains exclusive use of these items during the time the block lease is in effect.
Evolution of Reimbursement for Radiation Therapy
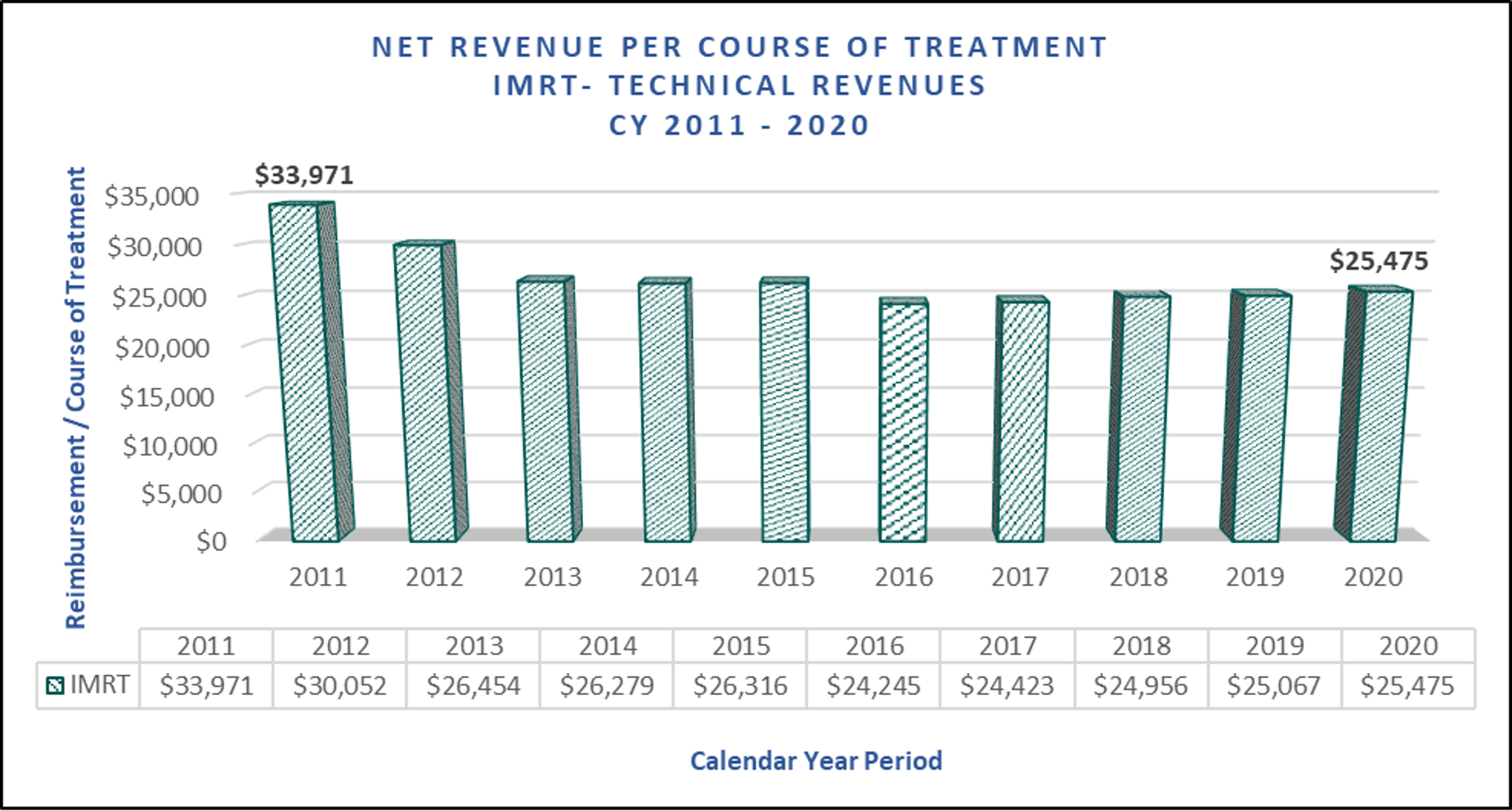
- Based on the product of the number of CPT units billed during a standard course of treatment requiring IMRT treatments multiplied by CMS’ technical reimbursement for these services in each year presented above.
- Does not consider impact of alternative payment models, non-Medicare, non-technical portions, or non-IMRT reimbursement.
It is informative to first understand where many providers stand today, before the CY 2021 reimbursement cuts take effect. The chart above provides a ten-year review of aggregate payment rates for a typical patient’s course of IMRT radiation therapy treatment. As can be seen, the Reimbursement trends during the past decade have not been highly favorable for Radiation Therapy Centers with a heavy reliance on Medicare payments and trends have been even less favorable to those that are primarily providing IMRT-based treatment options. The decade began with consecutive years of reimbursement cuts for IMRT procedures between 2011 – 2015. This would be followed by payment cuts occurring initiated in the CY 2016 MPFS as CMS made a permanent adjustment to the Equipment Utilization Rate (“EUR”) assumed for Linear Accelerators. This EUR is one of the key variables used in a specific formula by CMS to determine the level of payment for all providers using a given type of equipment and it’s increase, which was initially proposed to be shifted from 50% EUR to 75% EUR, would settle at 60% EUR, but still created a downward impact to reimbursement for radiation therapy providers. Since this time, payment rates for many radiation therapy procedures have been stagnant as a result of budget neutrality adjustments.
The overall impact of the reimbursement changes noted above caused the average total payment rates for IMRT-based treatment plans to decline by nearly $10,000 per course of treatment from $33,971 in 2011 to $25,475 in 2020. Providers with a large Medicare patient base which had entered the 2010’s with healthy profit margins have had to continually manage costs in order to navigate the last ten years successfully.
Capital Requirements in Radiation Therapy
Radiation Therapy businesses may be driven towards Block Lease Arrangements out of necessity as Radiation Therapy Centers are among the most capital intensive healthcare businesses and operational/start-up costs to open and begin operating this type of business are significantly outside the affordability of many aspiring owners without a substantial level of debt.
The most significant purchase or up-front cost for a particular radiation therapy facility is often the linear accelerator, as this is the primary equipment around which most free-standing radiation therapy businesses are built. The market for used linear accelerators has proliferated alongside a market for used parts, however, which often can be sources of much lower costs if contemplating a purchase. CMS recently shared their own survey data which would be used in the 2020 work RVU calculations utilized to determine reimbursement for procedures using linear accelerators. Responders indicated that they had spent an average of $2.82 million for a linear accelerator providing IMRT treatments.
There are other costs that must also usually be considered, however, such as CT Scanners used in CT Simulation, which can very quickly bring the price of equipment up as well. Last, and possibly most importantly, is the vault in which the accelerator is operated. The cost vary widely and will depend on what level of construction is necessary, but can easily reach into the hundreds of thousands for space and shielding for a single linear accelerator. This type of structure makes it difficult to move to any alternative location and though it is not necessarily the most costly investment, it can make changing locations more complicated than it would be for other types of businesses.
These initial start-up and equipment costs motivate both parties to move towards an agreement such as a Block Lease Arrangement. The Lessor may need additional sources of income to pay off the original debts incurred during the initial start-up phase. At the same time, the Lessee is driven by a desire to potentially avoid these same costs.
Block Lease Arrangements Explained
The schematic below provides an example of how a typical arrangement may be organized between lessee and lessors.
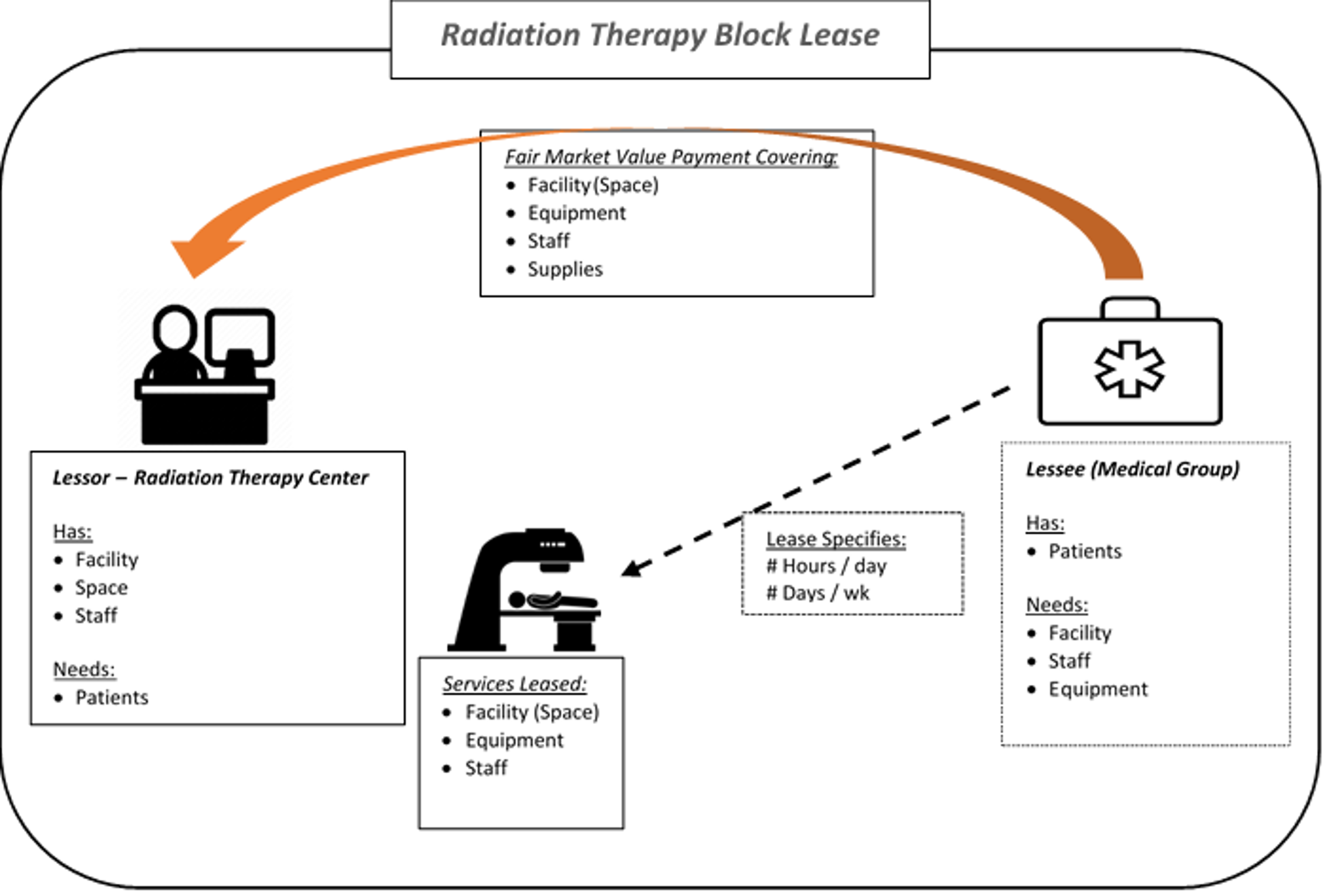
Block Lease arrangements are a less-aligned form of cooperation than an outright Joint Venture or practice acquisition with physician employment, however, they can generally achieve similar objectives for all participants involved. Within Radiation Therapy specifically, Block Leases involve owners of existing Radiation Therapy Centers (in this arrangement the “Lessor”) entering into an arrangement with outside providers such as a medical oncology group or other specialist group (the “Lessee”). Typically the Block Lease provides that facilities, personnel, and equipment are leased, supplies are provided, and the lessor continues to bill and collect on behalf of the lessee.
Depending on the legal / regulatory environment and the reimbursement environment, Block Lease Arrangements may provide a mutually beneficial solution to difficulties faced by each party while continuing to deliver quality and cost-efficient treatment services to the patients receiving care.
Block Lease Arrangements and Fair Market Value
Block leases may not always be referred to as a “Block Lease” and each can often be tailored to a specific situation or need but these agreements will generally involve the sub-lease of an existing radiation therapy operation to a third-party at a pre-determined rate, consistent with Fair Market Value. For regulatory purposes, the rate is always quoted in an official agreement on a per hour, or per unit of time basis and never on a per treatment basis. As noted previously, legal counsel should review structure for compliance with all laws and regulations.
The process of determining the Fair Market Value block lease rate begins with identifying the particular components that will be leased by the owner of the Radiation Therapy business to a third party. Most often, these components include equipment, facility space, non-physician staff, supplies, and other specified administrative and management functions which the lessor provides while the block lease is in effect. For a certain pre-defined time period, the third party will be utilizing each of these components and therefore, the third party must be charged for their use at a Fair Market Value rate.
These cost inputs used to calculate an overall FMV rate are individually built up and typically this is done using the actual cost historically incurred by the lessor. As is shown in the below diagram for staff costs, the build up accounts for the specific FTE wages and benefits to be included in the lease.
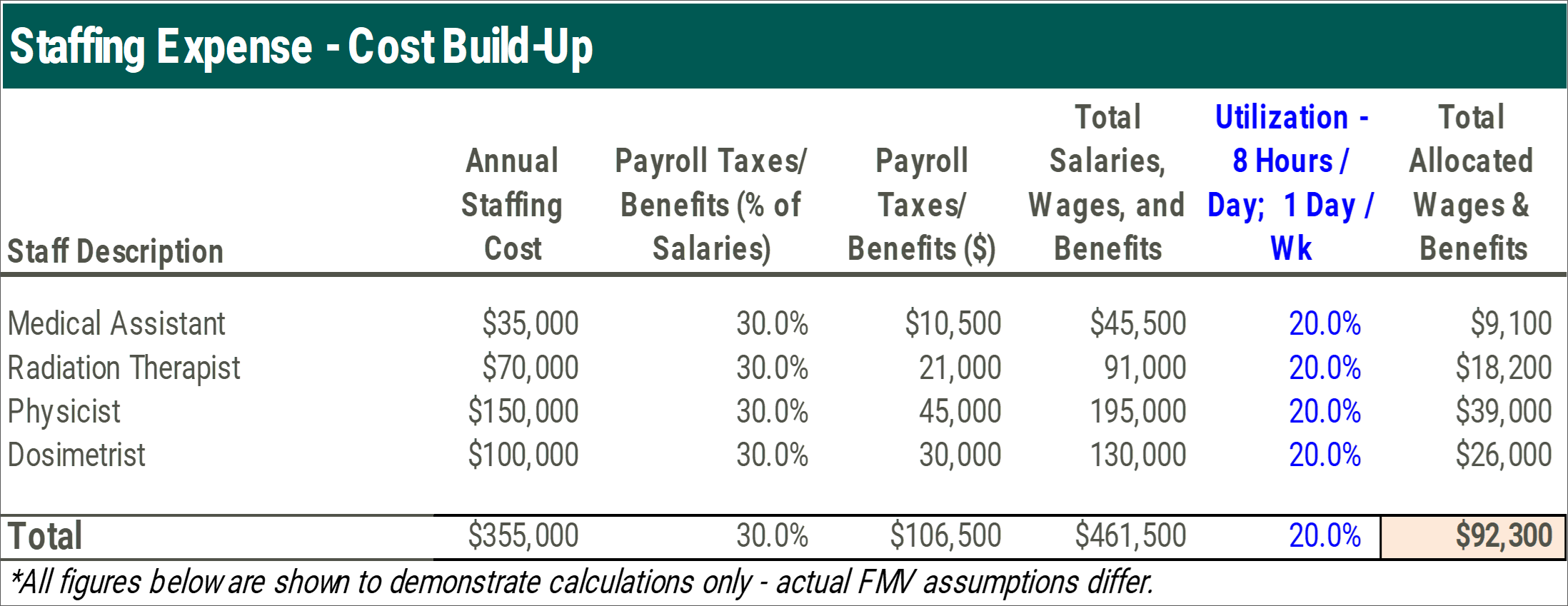
A key adjustment made in each cost build up is the utilization assumption, which takes into account the proportion of time that a particular cost is to be used by the lessee relative to the overall time which the cost is used. The above utilization rate of 20% would be consistent with a block lease in effect once a week for eight hours each day if the staff works a 40 hour, 5 day work week.
One of the primary components central to the block lease rate is the portion associated with the actual Radiation Therapy equipment which will be used in the block lease arrangement. The equipment is typically valued using an applicable fixed asset listing and equipment detail with consideration of equipment age, remaining life, make, and model. Equipment values are then used to estimate an annual lease rate applicable to the leased equipment. This lease rate is then adjusted for the utilization percentage for the Block Lease.
Facility or Space Costs are often estimated using allocation of costs stated in existing lease agreements and all other administrative or management costs applicable can be determined by identifying actual historical costs incurred by the current operator using available financial statements, management estimates, or contractual terms.
The chart below illustrates an overall cost build-up conclusion where each service provided by the lessor in a Block Lease is individually calculated based on the allocation of costs to provide the service. Adjustments are then applied to the base cost where a Mark-Up is appropriate. These mark-ups are not reflective of Fair Market Value and are presented for calculation purposes only. The sum of all costs with mark-ups is then used as a basis for the Cost Approach to determining Fair Market Value of a particular arrangement, which is then quoted in a range.
One important item not calculated or utilized to build up the costs below is the volume under the arrangement. These agreements should never be valued using a formula driven by expected patient treatment volumes or revenue for compliance purposes.
As the number of cancer patients continues to rise in the United States and Radiation Therapy continues to grow as a form of treatment, and further, as the regulatory and CMS reimbursement structure continues to evolve into the 2020’s, there will continue to be new types of arrangements that creatively address the issues faced by operators.
Sources:
- REPORT TO CONGRESS: Episodic Alternative Payment Model for Radiation Therapy Services (https://innovation.cms.gov/files/reports/radiationtherapy-apm-rtc.pdf)
- Linear Accelerator (LINAC) Price Guide & Costs(https://www.oncologysystems.com/resources/linear-accSelerator-guides/used-linac-price).
- ONCOLOGISTHOSPITALALIGNMENT (http://www.ccbdgroup.com/alignment2014.pdf)
- Finalized Policy, Payment, and Quality Provisions Changes to the Medicare Physician Fee Schedule for Calendar Year 2020 (https://www.cms.gov/newsroom/fact-sheets/final-policy-payment-and-quality-provisions-changes-medicare-physician-fee-schedule-calendar-year-1).
- CMS & Revenue Cycle Inc.
- org – 2021 MPFS final rule, E/M webinar today, PRO reviewer apprenticeships (https://www.astro.org/News-and-Publications/ASTROgram/2020/December-2020/ASTROgram_120220#:~:text=Yesterday%2C%20the%20Centers%20for%20Medicare,payments%20effective%20January %201%2C%202021.&text=For%20more%20information%20from%20CMS%2C%20see%20their%20final%20rule%20fact%20sheet)
- STARK AND MEDICARE’S PHYSICIAN REIMBURSEMENT RULES: UNRAVELING THE KNOTS https://www.gosfield.com/images/PDF/AGG.Stark_and_Reimb.PrePub_Draft.v2.011615.pdf





